
INTRODUCTION
Distal radius fractures are one of the most common upper extremity fractures.1 The primary goal of treating distal radius fractures is painless mobile wrist function through anatomic restoration of the articular surface and fracture stabilization.2
Surgical treatment options range from external fixation and percutaneous pinning to open reduction internal fixation with dorsal interlocking, fragment-specific, and volar locking plates (VLP). Currently, VLP is the most common treatment for unstable distal radius fractures.2 Locking plates act as a single rigid construct that supports stresses to subchondral bone without direct contact between the bone and plate.3 The locking mechanism increases stability, stiffness, and axial loading strength and allows for the fixation of reduced fragments in osteoporotic and comminuted bone.3 They also enhance early recovery of function compared to nonoperative treatment and reduce the risk of extensor tendon injury compared to dorsal plating.1,2
INDICATIONS & CONTRAINDICATIONS
Optimal management of distal radius fractures depends on the patient, fracture characteristics, and surgeon preference. Patient age, lifestyle, hand dominance, bone quality, and comorbidities are all factors considered when pursuing operative management. Acute distal radius fractures with post-reduction dorsal tilt >10°, radial shortening >3mm, intra-articular displacement, or step-off >2mm in patients younger than 65 may be indicated for volar plating.1 These guidelines can be expanded to include loss of reduction on subsequent radiographs, concomitant ulnar shortening >2-5mm, volar shear fractures, and volar ulnar corner fractures.2 Locking options extend the indications for volar fixation to include dorsally displaced fractures and those with anterior and/or posterior comminution.3
It is also imperative for the surgeon to recognize conditions in which VLPs would not provide the ideal construct. Dorsal rim fractures are difficult to capture from a volar approach. Fixation from a volar construct would require bicortical screws into the dorsal cortex, thereby increasing the risk of extensor tendon injury. Volar locking plates are also not designed to capture dorsal ulnar corner fragments, small sheared volar ulnar fragments, or avulsed radial styloid fragments.
SURGICAL TECHNIQUE
RELEVANT ANATOMY
Management of distal radius fractures requires a thorough understanding of the soft tissue and bony anatomy of the forearm and wrist. The volar approach to the distal radius begins with identifying surface anatomy such as tendons and bony prominences. The palmaris longus (PL) tendon lies in the midline of the volar wrist, just ulnar to the thicker flexor carpi radialis (FCR) tendon.
The palmar cutaneous branch of the median nerve usually arises proximal to the radiocarpal joint ulnar to the FCR tendon. The median nerve lies deep to the flexor digitorum superficialis (FDS) muscle, between the PL and FCR, and then enters the wrist through the carpal tunnel.
The radial artery lies below the volar fascia, immediately radial and dorsal to the FCR tendon. The superficial palmar branch of the artery lies close to the scaphoid tubercle and may be encountered during the dissection. The superficial radial nerve on the dorsal radial aspect of the wrist may be encountered with more lateral exposure, along with the first dorsal compartment, housing the abductor pollicis longus and extensor pollicis brevis. The flexor pollicis longus (FPL) tendon is deep to the FCR and passes through the carpal tunnel as the most radial structure. The pronator quadratus (PQ) is deep to the FPL, residing in the distal concavity of the radius.
The watershed line, used to determine the placement of the volar plate, is the osseous transition from concavity to convexity along the volar cortex of the radius.4 The articular surface of the radius has two facets for the scaphoid and lunate. The distal radius has an average volar tilt of 11° +/- 5°, radial height of 14mm +/- 1 mm, and radial inclination of 22° +/- 3°.2
SURGICAL APPROACH
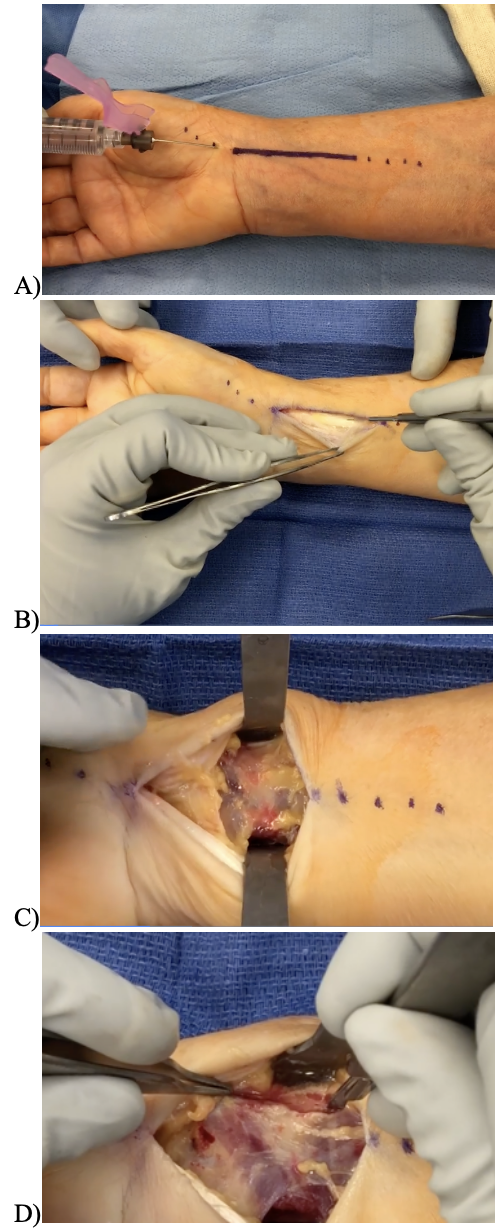
A longitudinal skin incision is made directly over the FCR tendon, extending from the proximal wrist crease into the distal forearm [Figure 1A]. Taking care to identify any branches of the palmar cutaneous branch of the median nerve, blunt dissection is performed down to the FCR tendon sheath. The FCR volar sheath is longitudinally incised, and the tendon is then retracted [Figure 1B]. The deep aspect of the tendon sheath is sharply dissected to expose the volar compartment. The FPL is retracted with the finger flexors ulnarly [Figure 1C]. The PQ is released radially and distally using sharp dissection and then reflected ulnarly using an elevator [Figure 1D]. The brachioradialis tendon can also be released using sharp dissection to aid in fracture reduction.
VOLAR LOCKING PLATE FIXATION
Extra-articular fractures may be reduced using traction and a volar-directed manipulation. Fractures with notable shortening may require a “shoe-horn” technique, where a Freer elevator is introduced between the fracture fragments to gently elevate the shortened distal fragment to a reduced position. Intra-articular fractures may require additional maneuvers. If the scaphoid and lunate facets are displaced relative to one another, the surgeon may reduce them in the same plane and maintain the reduction with a transverse radial-ulnar pin. Alternatively, the scaphoid facet can first be reduced to the radial shaft using a K-wire. Then, the entire unit can be approximated to the lunate facet as the forearm is pronated. Nascent malunions may require an extended approach, whereby the radial shaft fragment is pronated with a clamp to expose the dorsal aspect of the fracture. The dorsal periosteum can also be excised to mobilize the distal fragment if needed.
Once the fracture is reduced, a volar plate is placed along the shaft with adequate positioning and fit confirmed under fluoroscopy. The plate is applied to either the proximal or distal fragments first, depending on fracture characteristics and surgeon preference. With affixing to the radial shaft first, a screw is drilled through the oblong hole. The plate may be repositioned in the axial plane if needed before placing the distal screws. Alternatively, the distal fragment can be affixed to the plate first. The plate is then levered to the radius, whereby the volar tilt is corrected through the anatomic shape of the plate. The final plate and screw placement are confirmed using fluoroscopy [Figure 2]. Pearls and Pitfalls are addressed in [Table 1].


POST-OPERATIVE MANAGEMENT
Postoperatively, patients are placed in a soft dressing until their initial postoperative visit at 7-to-14 days. During this initial period, patients can use their hands for activities of daily living while focusing on the range of motion and edema management. However, they are restricted from performing strenuous or heavy tasks using the operative extremity.
At the initial postoperative visit, patients are transitioned to a removable wrist orthosis for protection and are educated on range of motion exercises. Strength and weight-bearing are generally allowed at six weeks.
DISCUSSION
Open reduction and internal fixation of distal radius fractures using VLP fixation provides immediate stability even in osteoporotic and comminuted bone.3 Osada et al. found that patients undergoing VLP with early mobilization for dorsally displaced distal radius fractures were highly satisfied at one year postoperatively, and all patients returned to activities of daily living and work.5
Despite overall good results, complications such as loss of reduction, intra-articular screw placement, and rupture of the flexor and extensor tendons may occur. Loss of reduction is usually caused by inadequate initial reduction or fixation. A working knowledge of the radiographic parameters and normal anatomy is critical in the reconstructive process. Restoration of the volar cortex restores the weight-bearing axis of the wrist. Fixation of the distal locking screws should be spread to support the articular fragments and placed into the subchondral bone for maximum support.2
Intra-articular screw penetration may occur directly from erroneous placement or indirectly from the subchondral collapse. Tangential views, in addition to standard AP and lateral views, can help avoid this complication. A skyline view can help assess dorsal screw penetration, while an oblique view can help detect intra-articular penetration.6 Lateral radiographs projected 23 to 30° of lateral tilt to match the radial inclination can also help ensure proper screw placement.7 Arthroscopic evaluation of the articular surface may also be a useful minimally-invasive tactic for evaluating screw position.
Tendon rupture most often occurs from increased contact pressures on the plate and tendon interface. Modern-day plates are now manufactured to be thinner with smoother edges. However, plate placement is critical: a plate placed too distal (over the convexity of the volar rim) has been shown to increase the risk of flexor tendon rupture.8 Additionally, long screws with dorsal protrusion risk injuring the extensor tendons. It has been demonstrated that a screw length of at least 75% of the bicortical distance of the distal radius can provide excellent stability while minimizing the risks of extensor tendon rupture associated with bicortical screws.9
Repairing the PQ over the plate is controversial in its role of preventing flexor tendon rupture. In theory, soft tissue coverage over the plate may provide a buffer to reduce contact pressures. However, a two-year prospective randomized trial showed no reduction in tendon irritation. The authors noted that PQ repair may be unreliable and should not be considered a fail-safe over a poorly positioned plate.10
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
This manuscript does not require ethical approval to report its findings.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.