

INTRODUCTION
Shin Splint is often a benign and self-limiting condition.1 There is a substantial variation in the choice of treatment. However, treatment recommendations start with non-operative modalities, including modification of activities, replacement of the shoe, ice in the acute phase, stretching and strengthening of the calf muscles, massage, and extracorporeal shockwave therapy, whereas surgical fasciotomy is reserved for recalcitrant patients.2,3
Different terms, including medial tibial stress syndrome (MTSS), stress fracture, chronic exertional compartment syndrome (CECS), periostalgia, and periosteal avulsion, have been used to better explain the pathophysiology; however, each of these has its distinct presentations. While CECS is not expected to show any abnormality in the imaging, bone stress fracture usually presents with focal and spindle-shaped cortical activity in the Technetium-99m-Methyl diphosphonate (Tc-99m-MDP) scan.4,5 Compared to a stress fracture, a faint heterogeneous linear uptake mainly extending along the lateral tibial cortex suggests a shin splint.5
Risk factors include a recent change in activity duration and intensity,6 female gender presumably because of the differences in muscle attachment,7 and anatomical abnormalities in the foot, including forefoot varus and decreased forefoot flexibility.8 Two systematic reviews on the risk factors in runners showed that a higher risk of shin splint is correlated with increased external rotation of the hip, female gender, orthotic use, being more novice in running experience, higher body mass index, and navicular drop.9,10
Management starts with prevention.11 Prior systematic review included four low-quality clinical trials assessing the role of shock-absorbing insoles, heel pads, Achilles stretching, proper footwear, and graduated running programs in preventing shin splints. This study did not find sufficient objective evidence to support the widespread use of either of the preventive measures. However, the shock-absorbing insoles were the only effective intervention that showed encouraging results. It seems reasonable that fatigued muscles cannot absorb the shock, resulting in the transmission of the ground reaction force to the bone-muscle interface.12 Moreover, it is intuitive that shoe wear replacement, especially after a certain running mileage, helps maintain the shock-absorbing feature as a preventive measure.13
CASE SCENARIO
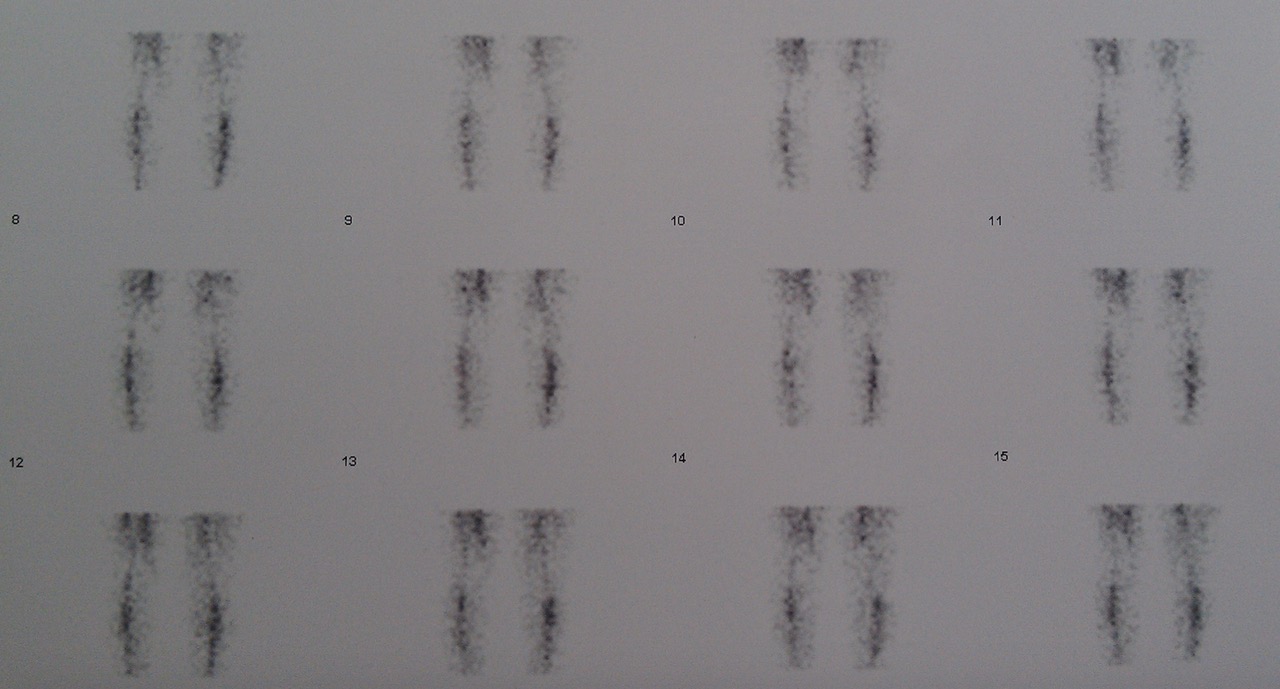
A 28-year-old woman developed pain in the left leg from 5 months ago. The patient indicated pain over the anterior compartment of the leg, more accentuated in the proximal area. It was activity-related but started with the activity over the bone, which was different from the chronic exertional compartment syndrome, which usually begins after 20-30 minutes of strenuous activity. The patient has had pain for more than five months. The examination revealed tenderness over the muscle bulk adjacent to the anterior tibial crest. The patient had a history of vigorous exertion that triggered the pain with no other health-related issues. Lower limb radiography was unremarkable. There was no clinically detectable genu varum or valgum. The bone scan confirmed the diagnosis of shin splint (medial tibial stress syndrome) by demonstrating linear uptake along the tibia in the delayed images [Figure 1a-c].



DISCUSSION
Little has been studied about the role of any intervention in the treatment course of shin splint until recently. Previously, shin splint treatment consisted of conservative modalities, including rest, ice, and activity limitation or modification. In recalcitrant cases, surgical fasciotomy was advised.2 A study comparing the effect of surgery on patients with and without increased compartment pressure, fasciotomy, and periosteal cauterization improved the symptoms in 93% and cured 78% of the patients with shin splints in whom the resting compartment pressure was normal.14 Although some studies have divided patients with leg pain into MTSS or CECS based on the compartment pressure, some reported pooled results regardless of the distinct diagnosis. Therefore, it is not clear whether patients with periostalgia and normal compartment pressure would benefit from surgery. Moreover, it is not clear whether any of these interventions are disease-modifying, palliative, or have a placebo effect.
A randomized clinical trial (RCT) compared four different nonoperative modalities with control. These modalities were phonophoresis in one group and iontophoresis in another group using dexamethasone and lidocaine, ice massage in group 3, and continuous ultrasound in group 4. All four groups showed higher pain relief than the control group, but neither one proved superior to the others, which might result from a placebo effect.15 In an RCT studying the effect of laser treatment compared to sham laser, it failed to show superiority over the control group.16 An RCT comparing ultrasound alone with ultrasound plus periosteal pecking (needling) showed comparable results.17 Another RCT comparing the graduated running program alone versus the graduated running program together with stretching and strengthening versus the graduated running program together with compression stockings did not show any significant difference between the different treatments.18 Leg brace versus no brace was studied in 3 RCTs and subsequently pooled in a systematic review, concluding that there was no difference in pain and return to duty with a brace.17 Pulsed electromagnetic field was used in an RCT compared to placebo, which showed no difference with respect to pain.17 Extracorporeal shockwave therapy (ESWT) was studied in 2 non-randomized controlled trials.19,20 Both studies showed improvement with more athletes returning to sports after having ESWT, which was also supported after pooling the data in a systematic review.17 This was the only treatment effective in shin splint; however, both studies were non-randomized with low-quality design.
Massage, together with stretching and strengthening, is recommended to help relieve pain. To avoid further traction injury during massage, a broad and light massage should be exerted transversely with respect to the soleus muscle fibers rather than a deep digital ischemic pressure massage.21 Corticosteroid injection is another nonoperative treatment commonly used for tendinopathies to relieve pain, which has not yet been studied in an RCT for treating shin splint; however, it does not seem to modify the disease. Instead, it might increase the number of patients requiring surgery, as shown in upper extremity tendinopathies.22 Moreover, it was reported to develop skin atrophy and depigmentation with no positive effect on shin splint pain.2
Despite the many papers published about shin splints and MTSS, most have looked at the risk factors and contributing causes rather than the treatment. Only sporadic low-quality RCTs are available in the literature, with insufficient data to support a treatment. Yet there is a shortage of evidence for the best treatment option, with most available treatments based on experience. No one of the randomized studies proved the superiority of the intervention over the placebo.23 Massage is widely used, but there is no clear evidence to match the type of massage with the mechanism of injury based on the proposed theories. The only evident effective treatment was ESWT based on two non-randomized and low-quality studies.24 Considering the shortcomings of evidence for the treatment of shin splint and a substantial variation in the treatment options, it is necessary to design higher quality RCTs to compare the treatments with placebo.
Medial Tibial Stress Syndrome or Shin Splint should be considered a differential diagnosis. Since the interventions differ from chronic exertional compartment syndrome, a correct diagnosis via additional imaging is necessary to avoid treatment failure. It also seems to be a self-limited benign condition that does not accumulate with age, in contrast to conditions that do accumulate with age, such as arthritis.3 This is shown in tendinopathies of the upper limb and can be generalized to any tendinopathy or periostalgia in the limbs. This suggests that not every patient with this condition requires treatment. The substantial variation in the treatment options indicates that physicians have undue influence on the treatment choice. For discretionary treatments for benign conditions like shin splints, patients may benefit from easy-to-understand, balanced, dispassionate information about their disease and the options for treatment. This information is often referred to as a decision aid.25 Future research should address the ability of decision aids to decrease surgeon-to-surgeon variations in treatment and ensure that the patient’s values and preferences have a central role in decision-making.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval
This study does not require ethical approval
Declaration of informed consent
there is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.