
INTRODUCTION
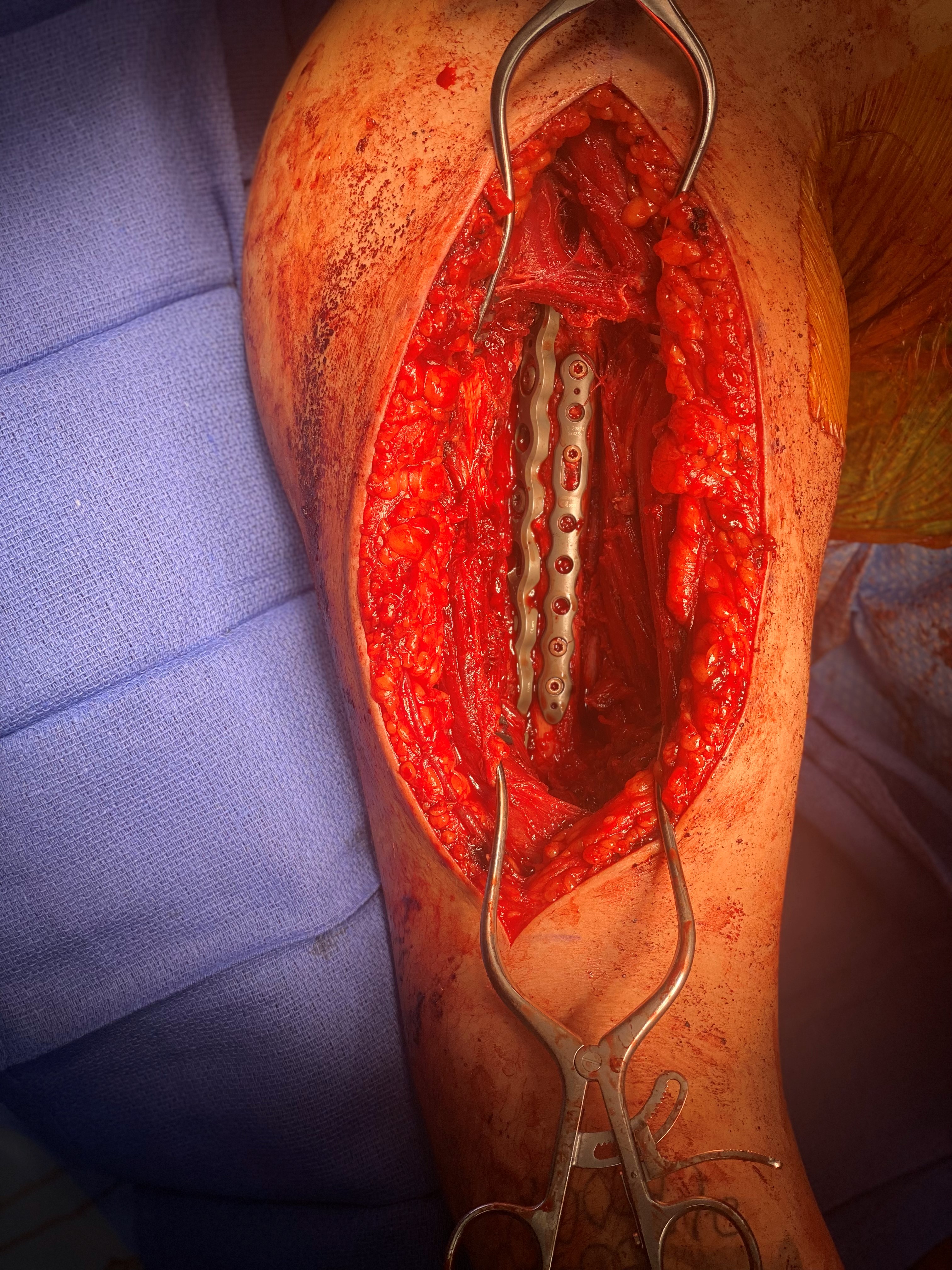
Open Reduction and Internal Fixation (ORIF) is the most common method of providing operative stabilization of humeral shaft fractures.1 The treatment choice can be performed through numerous approaches addressing various injury characteristics (i.e., fracture pattern, soft tissue injury, radial nerve damage, etc.) Recent biomechanical studies have shown the added strength of a second plate applied to the shaft.2–4 A single plate is typically used for ORIF of humeral shaft fractures [Figure 1].

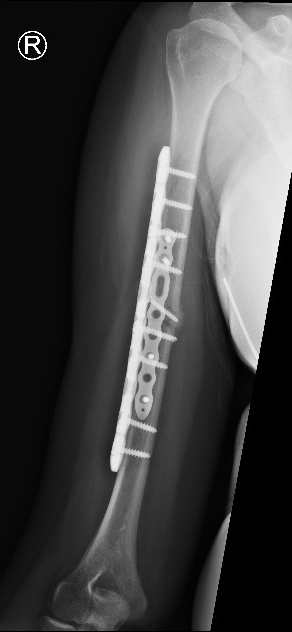
The second plate, whether orthogonal or in parallel, increases stability and reduces the risk of hardware failure prior to healing [Figure 2, Figure 3].5 Although there is evidence for the benefits of ORIF, there is limited data on how plate number and size may affect outcomes such as union rate, pain scale, and other complications.6–8 There may be added implant costs to adding a second plate to a humeral shaft fracture, but we know of no specific contraindications. This study compares the radiological and surgical outcomes of single and dual-plating techniques. Our primary null hypothesis was that there is no statistically significant difference in the union rate between single versus dual plating for humerus shaft fractures. Our secondary hypothesis is that there is no significant difference in the rate of complications and pain level between single and dual plating.


METHODS
A retrospective review was performed at a single institution. Between March 2010 and May 2022, 365 patients with humerus diaphyseal fractures were treated with either single or overlapped dual-plate ORIF in an orthogonal plate configuration. Seven fellowship-trained surgeons at a Level 1 trauma center were involved in this study, and the choice of single or dual-plating was at the discretion of the treating surgeon. The most common indication for ORIF of the humerus was polytrauma. Other common indications included failure to maintain acceptable alignment with closed treatment and open fractures. All fractures were classified using the Arbeitsgemeinschaft für Osteosynthesefragen/Orthopedic Trauma Association (AO/OTA) classification system and were all 12A, 12B, or 12C type fractures.
Patients were excluded based on the following criteria: (1) under 18 years of age, (2) lost to follow-up, (3) tumor-related pathologic fractures, (4) fractures around a periprosthetic implant or previous ORIF plate, (5) revision cases for re-injury within 12-month follow-up period and (6) duration of injury date to surgery of over 90 days. After the exclusion criteria, 143 patients were included in the study.
All data were collected through our hospital data system and categorized by patient demographic characteristics, injury characteristics, intra-surgical variables, and surgical outcomes.
Patient demographic characteristics included age, sex, body mass index (BMI), obesity (BMI over 30.0), type I or type II diabetes, osteoporosis (taken from electronic medical records), and tobacco use (current, never, former).
Injury characteristics included the mechanism of injury, closed/open fracture, multiple fractures, polytrauma, AO/OTA fracture classification, associated radial nerve injury, and previous humerus shaft fracture of the affected arm. The mechanism of injury was divided into four categories: low impact (e.g., fall from standing height), high impact (e.g., motor vehicle crash, motorcycle crash, pedestrian struck by a vehicle, fall from height), gunshot wound, and other (physical altercation, sports injury, crush injury). Polytraumas were defined as injuries to multiple body systems, and multiple fractures were defined as any trauma that involved a fracture to the humerus shaft and another bone. The fracture classification and location were assigned based on pre-injury radiographs. Each radiograph was assigned a classification by an orthopaedic physician.
Intra-surgical variables included time from injury to surgery (days), length of surgery (minutes), number of concurrent procedures performed during the humeral shaft ORIF (i.e., ORIF of other fractures, complex skin closure, neurolysis of the radial nerve, irrigation, and excisional debridement, etc.) estimated blood loss, use of lag screws, number of screws implanted, and plate metal type (titanium or stainless steel).
Surgical Outcomes included visual analog scale (VAS) score during the final follow-up visit, length of time between surgery and final follow-up visit, failure to union at six months, failure to union at twelve months, hardware failure requiring corrective surgery, postoperative radial nerve injury, and post-surgery infection requiring irrigation and debridement. Hardware failure included implant deformity and symptomatic hardware. Fracture union was defined as a bridging callus on three out of four cortices of the fracture line. To determine fracture union sequential radiographs at 3, 6, and 12 months after surgery, radiographs were examined by an orthopaedic surgeon.
Data values are expressed as mean (standard deviation) for continuous variables and count (%) for categorical variables. Two-sample independent t-test (or Wilcoxon rank sum test) was used to compare continuous variables, while the Chi-square test (or Fisher exact test) was used to compare the distributions of categorical variables between patients with dual-plating and single-plating. All analyses were done using Statistical Analysis System (SAS) 9.4, and conclusions were made at a 5% significance level.
The Institutional Review Board approved this retrospective study. Data were collected from medical records and de-identified.
RESULTS
The patient demographic characteristics are categorized into single (79 patients) or dual-plating (64 patients) groups [Table 1].
There were 81 females and 62 males included in the study. The average age was 47.3 years, ranging from 19 to 90+. Between the single and dual-plate groups, dual-plating treated a significantly higher number of patients with osteoporosis. There was no statistically significant difference in any other patient demographic variables. [Table 2]
Among the intra-surgical variables and plate characteristics, time to surgery, use of lag screws, length of surgery, number of concurrent procedures, and estimated blood loss showed no significant difference between groups [Table 3 & 4]. As expected, dual-plating showed a significantly higher number of screws used. Most of the plates used in single-plating were constructed out of stainless steel, while nearly all the plates in the dual-plating group were titanium.
There was no significant difference in any of the surgical outcomes between single and dual-plating. Nonunion occurred within six months in 8% of the patients (n=143) and at twelve months in 2% of the patients (n=130). The single-plating groups had five hardware failures (6%) and two post-surgery infections (3%). In this group, five cases of hardware failure (6%) and one case of infection (1.5%) required subsequent revision surgery. The dual-plating groups had three hardware failures (5%) and three post-surgery infections (5%). In the dual plating group, three cases of hardware failure (5%) and three cases of infection (5%) required subsequent revision surgery. Postoperative radial nerve injury was recorded in 2% of the patients, three from single-plating and two from dual-plating. [Table 5]
DISCUSSION
A comparison between our single-plate and dual-plate groups shows no significant differences in any of the surgical outcome variables. (i.e., failure to union at 6 or 12 months, hardware failure, postoperative radial nerve injury, and infection) Each group’s surgical outcomes fell within the range of the reported literature.9–17 Our study shows that dual-plating may be considered a comparable viable surgical option. The dual plating group had a fracture union rate of 98% at twelve months. We observed no differences in the intra-surgical complications and post-surgical complications (failure to union, hardware failure, postoperative radial nerve injury, or infection). The five postoperative radial nerve injuries (three single plate, two dual plate) recovered within six months.
Dual plates were more likely to be used in osteoporotic and low-energy injuries. Among the low-energy injury patients diagnosed with osteoporosis, 13 underwent dual-plating fixation, while only four were treated with single-plating. Removing patients with osteoporosis removed the significance between the mechanism of injury groups (p-value 0.162) and did not significantly affect any other variable. Separately, gunshot wounds as the mechanism of fracture were more likely to receive a single plate for the fracture, mainly due to the single plate approach bridging the fracture. Conversely, the dual plating technique would reduce the fracture pattern anatomically.
If single-plating seems to perform as well as dual-plating in this study, why do we see a trend of increased usage of dual-plating for ORIF of a humeral shaft fracture? First, as discussed, we know that it is biomechanically stronger. The increased strength of the construct may provide reassurance with early weight-bearing through the arm, especially in polytrauma patients where crutch weight-bearing is important. In vitro, biomechanical models suggest that dual-plating is mechanically superior (stiffness and fatigue resistance) to a single-plate construct.18–20 Second, the dual-plate construct may be technically easier to insert. A provisional smaller plate allows for an easier application of a larger definitive plate because it maintains the reduction when adding the larger definitive plate. Third, a planned application of dual-plating ensures enough biomechanical strength for a fracture that may be more transitional between the shaft and the meta-diaphysis, wherein dual-plating has been shown to be superior.21 Fourth, recent literature has demonstrated that dual-plating leads to a lower nonunion rate.22 Among these factors, other important considerations in deciding between single and dual plating include the need for bridge plating due to comminution and the location along the humeral shaft, whether diaphyseal or meta-diaphyseal. These findings can imply that using dual-plating removes the decision-making of single versus dual-plating and protects in case dual-plates were appropriate.
There are several limitations to this study. First, dual-plating may have some advantages, as discussed. Still, a randomized, prospective study is recommended to elucidate further any differences between using single or dual-plating for ORIF of a humeral shaft fracture. Second, seven different orthopaedic surgeons with varying techniques performed the surgeries utilizing a variety of plates. Third, heterogeneous etiologies of fracture types, including open fractures, were included in the study, which can make comparison challenging. Finally, no functional outcomes were collected in this study, relying retrospectively on fracture union as the primary endpoint. Follow-up studies should examine clinical outcomes of different dual-plate combinations (i.e., length combination, width combination, plate material, etc.) Further biomechanical studies on the implant material, stainless steel, and titanium suggest that stainless steel has a higher stiffness and fatigue life than titanium plates, potentially allowing for a better clinical outcome in certain fracture patterns.23
CONCLUSION
In conclusion, in this retrospective series of humeral shaft fractures, we found dual-plate fixation for ORIF of humerus shaft fractures to be no statistically significant difference compared to single plate fixation. Dual-plating has satisfactory radiograph and clinical outcomes compared to conventional single-plate fixation. While we are not advocating for the routine use of dual-plating, our study’s results suggest that dual-plating results in similar outcomes as single-plating for ORIF of a humerus shaft fracture. Further studies are recommended to define better the indications for dual plating of humeral shaft fracture. Patient factors such as osteoporosis may be important to explore.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
Ethical approval was obtained by the Cooper University Health Care Institutional Review Board (IRB# 21-205) on December 13, 2021.
Declaration of informed consent
There is no identifiable information included in the submitted manuscript that can be used to potentially identify study subjects.
Acknowledgments
We would like to acknowledge Julio Rodriguez, MD and Karnesha Goins, MD who have not met the criteria for authorship, but we would like to acknowledge for their efforts.