1. Introduction
Rotator cuff (RC) tears are one of the most common tendinous injuries seen in the adult population,1 accounting for 5.7 million annual office visits in the United States alone.2 The glenohumeral (GH) joint has the largest range of motion of any joint in the human body. Consequently, it is susceptible to injury when subjected to high stress, extreme range of motion, or repetitive use.3 The supraspinatus plays an important role in the dynamic stabilization of the GH joint and is the main muscle-tendon unit during abduction.4–8 Subsequently, it is the most vulnerable structure commonly affected by injury and degeneration.9–13 One of the factors causing RC tears is intrinsic tendon degeneration,14 caused by increased strain on the tendons, which can lead to tear progression.15 A comprehensive understanding of the biomechanical properties of the RC is valuable for understanding the risk of injury and progression, rehabilitation, and surgical treatment.
RC treatments aim to return function, reduce pain, and restore the mechanical environment of the RC tendons. After RC repair, early passive motion is a standard rehabilitation protocol to avoid postoperative stiffness and help regain function by strengthening the mechanical environment.16 Common rehabilitation exercises to treat patients non-operatively involve abduction of the arm to strengthen the supraspinatus, which plays a vital role in this motion.11,17 However, non-operative management can result in tear progression, and surgical management can result in subsequent retear.18–21 A better understanding of the heterogeneous mechanical environment and spatial strain on the supraspinatus tendon during its dynamic motion could lead to targeted patient management based on tear characteristics and the mechanical properties of the supraspinatus tendon.
The accurate simulation of the supraspinatus mechanical behavior has proven difficult and is most often simulated during static positioning at discrete abduction angles.22–24 Bey et al.22 evaluated the spatial material properties throughout the supraspinatus tendon at GH abduction angles of 15°, 30°, 45°, and 60°, showing that strain significantly increased as the abduction angle increased, and the bursal side of the tendon experienced significantly greater strains than the articular surface. Huang et al.23 performed static uniaxial tensile tests on the supraspinatus tendon at GH abduction angles of 22°, 63°, and 90°, confirming that the bursal surface experiences greater strains than the articular surface. However, they found that the articular surface strain decreased with increasing angle, compared to the bursal-sided strain increasing with abduction angle. Miyamoto et al.24 evaluated the internal strain of the supraspinatus tendon at different elevation angles. They found that at 20° and 30° of abduction, the strain was significantly higher compared to -10° and 0° of abduction. Conversely, Riley et al.25 found that the strain on both the articular and bursal sides increased with increasing abduction angle; however, the articular side experienced more strain. Furthermore, they produced the only study that compared the differences in strains at the anterior and posterior tips of the supraspinatus tendon but found no significant differences.
While these studies glean insight into the heterogeneity of the mechanical environment of the RC, they do not represent tendon behavior during physiologic motion, as they do not account for the dynamic nature of the GH joint nor the contribution of the other RC muscles during abduction, thereby limiting clinical application. This study aims to evaluate the biomechanical properties of the supraspinatus tendon during abduction to account for the dynamic nature of the GH joint and load-sharing interactions between the RC tendons. This will allow for a more robust understanding of the mechanical environment of the supraspinatus tendon for decision-making in supraspinatus injuries. Furthermore, we aim to explore the region-specific strain response of the supraspinatus tendon to better understand the differences in local deformation and determine whether different regions have different strain patterns. Previous literature has generally looked at the average tendon strain. However, there may be region-specific responses. In this investigation, we employed a validated, cadaveric shoulder testing system26–28 and used joint motion definitions recommended by the International Society of Biomechanics29 to study joint mechanics. We hypothesize that during abduction, the posterior region of the supraspinatus tendon insertion will experience the highest strain.
2. Methods
2.1. Sample Preparation
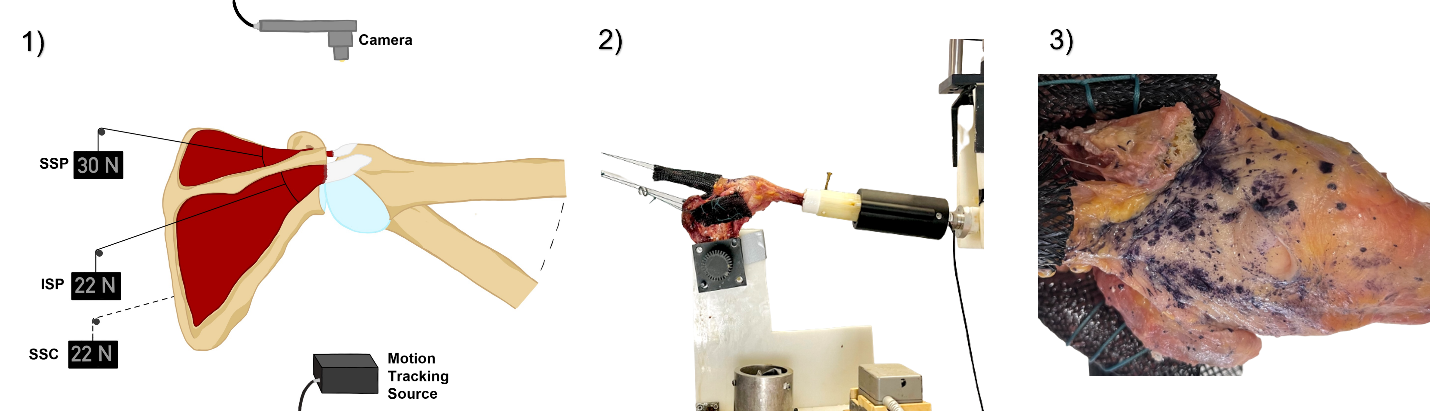
Five fresh-frozen intact human shoulders were acquired (Medcure, Inc., Providence, RI, USA), with an average age of 56.7 ± 6 years, a height of 5’ 6’’ ± 3’', and a weight of 147.3 ± 23 lbs. There were no visible signs of RC tears, fraying, or delamination in the RC tendon specimens; thus all specimens were included for data analysis. Care was taken to maintain the integrity of the GH joint capsule and the RC during all specimen dissections. The skin and the muscles were removed, excluding the supraspinatus, infraspinatus, and subscapularis muscles. The clavicle was disarticulated at the acromioclavicular joint, and the distal acromion was removed. The RC muscles were dissected free of their origins, and the free ends were sutured between a 1mm diameter polyethylene terephthalate (PET) expandable braided sleeving (TechFlex, Sparta, NJ, USA) using a Krackow stitch. The shoulder was mounted in a custom 3-dimentional (3D) printed polylactic acid (PLA) component of the validated testing system by rigidly fixing the scapula while the center of the glenoid and the superior and inferior angles of the scapula aligned with the vertical plane [Figure 1].28,30 The scapula was titled 30° upward relative to the vertical31 and then tilted 10° anteriorly to mimic the physiologic resting position of the scapula.32–34 A two-part epoxy cast was then used to secure the scapula in place (Smooth-Cast 300q, PMC Smooth-on Inc., Macungie, PA, USA). Similarly, the humerus was potted into a custom 3D-printed component of the validated testing system.28,30 The surface of the supraspinatus tendon was then sprayed with a hematoxylin stain to create a speckle pattern that was used to assess tendon strain via digital image correlation.
2.2. Testing System
A previously validated testing system able to prescribe motion with an absolute percent error of 0.9%26,27,35,36 allowed for the actuation of the major RC muscles (Infraspinatus, Subscapularis, and Supraspinatus) during isolated GH abduction28,30 [Figure 1]. Each of the RC muscles was connected to a tensile load cell (LCM300, 50 lb., Futek Advanced Sensor Technology, Inc., Irvine, CA, USA) with two springs in parallel and a bipolar stepper motor (Nema 23, Gear Ratio 47:1, StepperOnline, Nanjing City, China). A two-piece humeral slide mechanism between the humerus and the testing system allowed for abduction introduced by the testing system arm. A custom matrix laboratory (MATLAB) script employed a proportional force feedback control loop, updated at 10 Hz, to ensure the correct load was applied to the tendons during GH abduction. A complementary metal–oxide–semiconductor (CMOS) microscope camera (PL-D753-CU, Pixelink, Navitar, Rochester, NY, USA) was positioned directly above the humeral head and supraspinatus tendon [Figure 1] to capture the deformation of the tendon as the GH was abducted. Overall, the scapula was fixed, the humerus was passively abducted by the testing system arm, and the supraspinatus tendon insertion was tracked.
_cadaveric_testing_system_set_up._the_electromagnetic_position_and_orientation_data_col.png)
2.3. Motion Analysis
Using an electromagnetic motion tracking system (Liberty, Polhemus, Colchester, VT, USA), reference points on the humerus and scapula, according to the International Society of Biomechanics guidelines,37 were recorded at approximately 90° of GH abduction in the scapular plane. These points were used to create the humerus and scapula coordinate systems37), and a custom MATLAB script was used to calculate and display the GH angles in real time. This allowed for precise specimen positioning during testing.
2.4. Testing Conditions
The RC muscles were attached to the stepper motors by high-strength polyethylene cord and a series of eye hooks in the following manner: the supraspinatus line was adjusted to form a 10° angle with the horizontal; the subscapularis line was adjusted to an angle bisecting the lateral margin and the spine of the scapula ventrally; and the infraspinatus/teres minor line was adjusted in the same manner as the subscapularis, but dorsally.28 This allowed for loading the muscles along their physiological lines of action [Figure 1.2].33 To account for the load-sharing interaction between tendons, a constant 22-newton force was applied to the infraspinatus and the subscapularis.38,39 A 30-newton load representing approximately 26% of the force generated during maximal GH abduction was applied to the supraspinatus tendon.22,40 Our programmable testing system arm26 abducts the GH joint from 60° to 90°, supported by findings by Kim et al.41 that in-vivo strains are the highest at 90° of abduction. The stepper motors were adjusted by the proportional force control feedback loop to apply load to each RC muscle throughout the arc of GH motion according to the desired muscle activation profile.
2.5. Data Acquisition
With the feedback of the anatomical coordinate systems and the motion provided by the programmable testing system arm,26 the humerus was raised in the scapular plane from 60° to 90° of GH joint abduction for two repetitions after a single preconditioning cycle. To protect the specimens, testing was performed at a reduced speed (duration of abduction motion: 28 s).28,30,35 During testing, the shoulder specimens were repeatedly inspected to ensure the RC and joint capsule’s integrity and maintenance of moisture with 0.9% saline.28,38,42–44 The electromagnetic motion tracking system recorded the three-dimensional position and orientation of the humerus and scapula sensors. The CMOS microscopic camera was set to record images of the supraspinatus tendon insertion at each degree (0.93 Hz) of GH abduction to assess strain by digital image correlation.
2.6. Data Analysis
2.6.1. Supraspinatus Tendon Insertion Strain
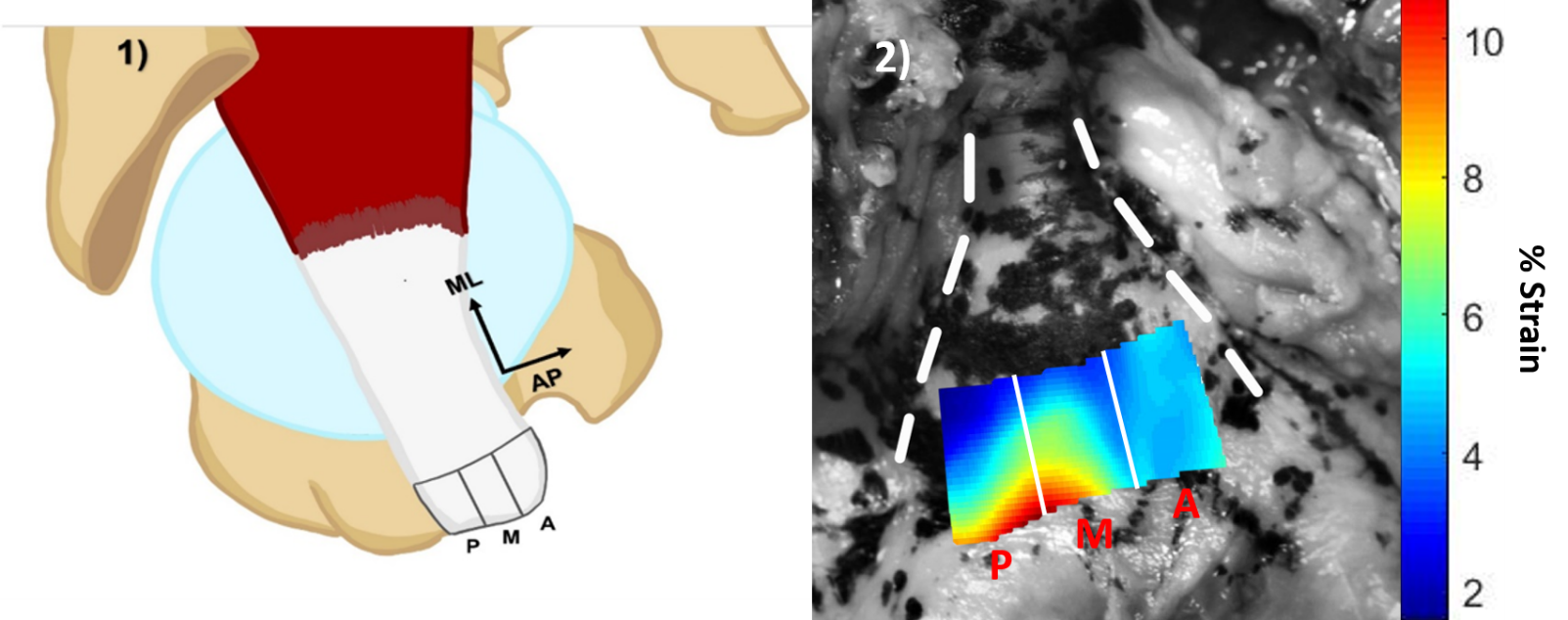
Optical measurements of surface deformation and digital image correlation (NCorr)45 were used to estimate medial-lateral (ML) and anterior-posterior (AP) directional [Figure 3.1] surface strains at the supraspinatus tendon insertion spanning the entire AP width of the tendon and approximately 2 cm in the ML direction to capture the critical zone of the tendon insertion where tears most commonly.46 Using an open-source digital image correlation program (NCorr C++ Port), the speckle pattern on the surface of the supraspinatus tendon insertion from the hematoxylin stain was tracked for the full sequence of images during abduction from 60° to 90° and the resulting Eulerian strains in the ML and AP directions were estimated.45 An in-house developed code (MATLAB 2019a, MathWorks, Natick, MA, USA) was employed to estimate maximum principal surface strains from the ML and AP directional strains at the supraspinatus tendon insertion [Figure 2.2[, which was then split equally into three regions: Posterior, Middle, and Anterior. The strain in each region was then averaged to obtain a single value used to compare regions.
_right_shoulder_supraspinatus_tendon_insertion_outline_by_the_black_box__morphologically.png)
2.6.2. Statistical Analysis
A Shapiro-Wilk test was used to assess the normality of the data. The students’ paired t-test was performed to ensure that the shoulders donated from the same specimen behaved differently and could be considered individual specimens for further analysis. A simple linear regression was used to determine the effect of abduction angle on tendon strain. Data were analyzed using a one-way repeated measure analysis of variance (ANOVA) at each abduction angle for the three regions (Anterior, Middle, and Posterior) considered within-subjects factors. The Tukey post-hoc test followed analysis for multiple comparisons of simple effects of the region on percent strain within each abduction angle. Statistical analysis was performed using GraphPad Prism unless otherwise noted (version 9.3.1 for Windows, GraphPad Software, San Diego, CA, USA). Two-tailed P values less than 0.05 were considered significant.
3. Results
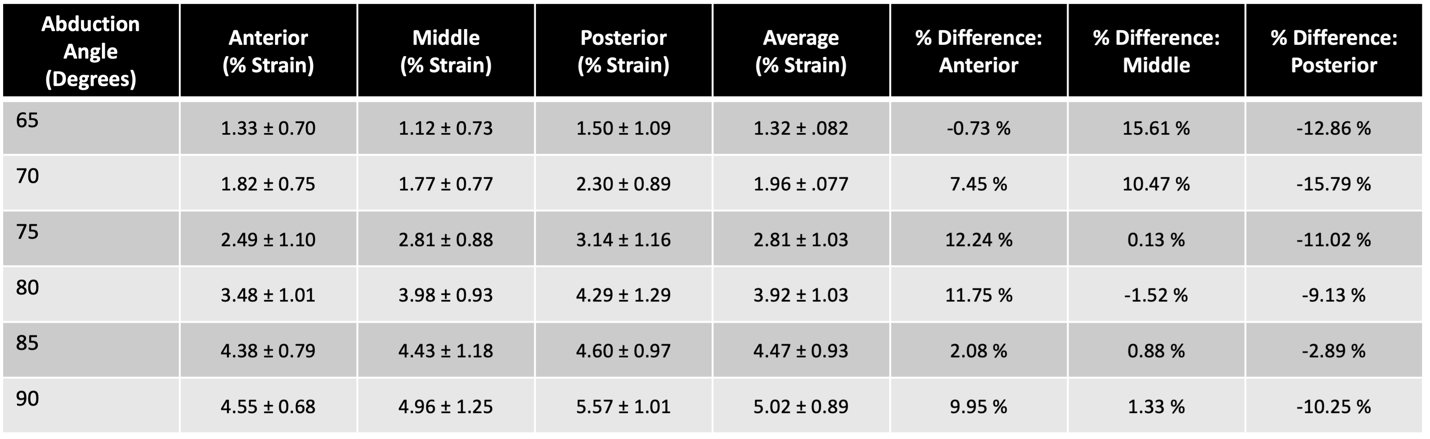
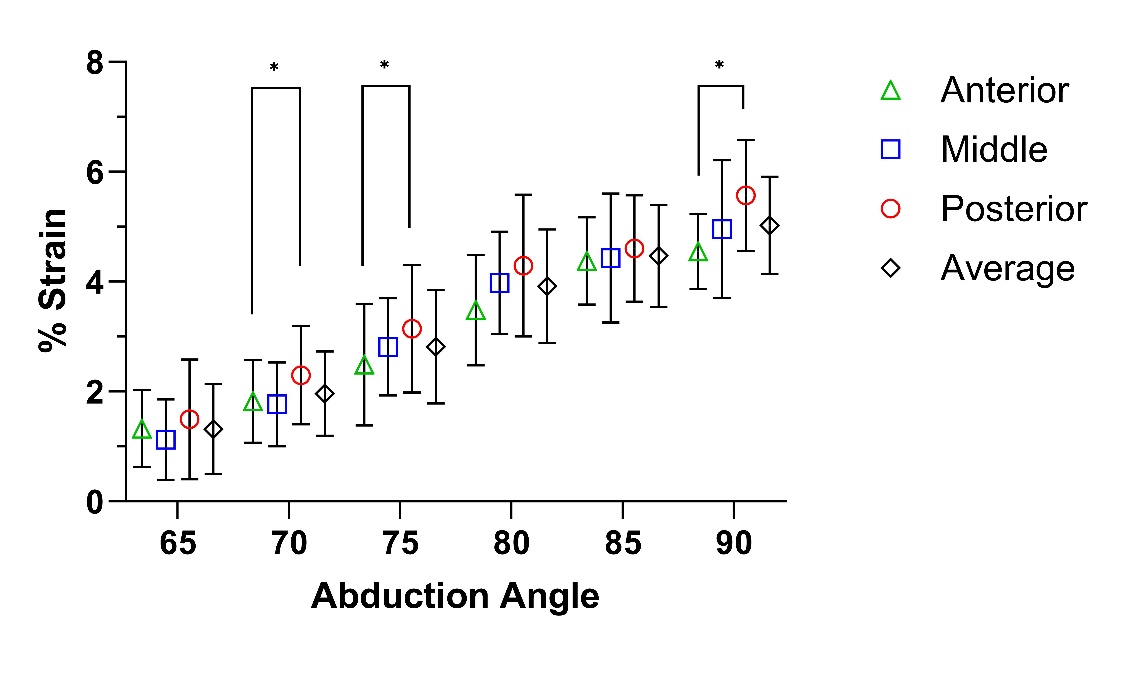
The supraspinatus tendon strain increased with increasing abduction angle for all regions tested (Anterior: R2 = 0.70, Middle: R2 = 0.70, and Posterior: R2 = 0.67) with the peak strain occurring at 90° of GH abduction [Figure 3]. The average values of peak strain (90° of GH abduction) were 4.54 ± 0.68, 4.96 ± 1.25, and 5.57 ± 1.01 percent for the anterior, middle, and posterior regions, respectively [Table 1].


The posterior region of the supraspinatus tendon insertion exhibited significantly higher strain than the anterior region at 70° (P = 0.037), 75° (P = 0.028), and 90° (P = 0.011) of abduction [Figure 3]. Comparing the average tendon strain to the different regions showed that the average strain will overestimate the anterior regional strain (max percent difference of 12.24%) and underestimate the posterior regional strain (max percent difference of -15.79%) [Table 1]. Identifying the regional strain response allows for a more comprehensive evaluation of the supraspinatus tendon’s mechanical environment by identifying how different regions behave during simulated abduction.
4. Discussion
In light of our cadaveric study investigating the impact of GH abduction on supraspinatus tendon strain, our findings provide valuable insights into the mechanical behavior of this critical shoulder structure. Our results demonstrated a clear association between GH abduction and supraspinatus tendon strain, with strain levels steadily increasing as the abduction angle progressed with the maximum strain level at 90° of GH abduction. The central focus of our investigation was the observation of strain variations across different regions of the supraspinatus tendon as a function of abduction angle. Our analysis revealed notable regional disparities within the supraspinatus tendon with distinct strain patterns in the anterior, middle, and posterior regions; the posterior region consistently exhibited substantially higher strain levels than its anterior counterpart at abduction angles of 70°, 75°, and 90°. This discrepancy challenges previous studies that have reported average strain values across the entire supraspinatus tendon,22,24,47,48 suggesting that such an approach may lead to overestimating strain in the anterior region and underestimation in the posterior region.
Due to the structural and mechanical heterogeneity of the supraspinatus tendon,23,49,50 RC tear pathology is poorly understood and difficult to manage. The supraspinatus is critical in arm abduction and stabilizing the GH joint throughout all ranges of motion.51 Thus, understanding the mechanical environment of the supraspinatus during various ranges of motion is of great interest. Previous studies that have examined the mechanical environment of the supraspinatus tendon have not accounted for the varying regions within the tendon and found the tendon strain as the average of the entire insertion, limiting the ability to fully understand the mechanical environment.22,24,47,48 At static abduction angles, Huang et al.23 found a significant increase in the bursal surface strain with increasing abduction angle from 22° to 90° at the osteotendinous insertion. Reilly et al.25 measured strain at the anterior and posterior edges of the supraspinatus tendon and saw no significant difference in the regional material response. On the other hand, our study examined the strain across the surface of the entire tendon insertion and found that as load and abduction angle increase, the posterior region exhibits larger strain than the anterior region. This discrepancy in results could stem from the difference in strain measurement techniques, the static position of the GH joint, or the loading of the other RC muscles. Reilly et al. used miniature DVRTs, which require inserting pins into the tendon. This may alter tissue strain measurements based on the tendon length where the DVRT was affixed. To capture the full 2D strain field of the supraspinatus tendon insertion, we used digital image correlation, which has been shown to capture strain within a 5% difference from conventional methods,52 allowing a more comprehensive evaluation of the entirety of the surface.
It should be noted that the surface strain reported in this study is much higher than in studies that have used similar loads. This could be explained by the differences in strain measurement techniques described previously or by the loading of the infraspinatus and subscapularis, which have been shown to interact mechanically with the supraspinatus.38,39 Previous studies, such as Miyamoto et al.,24 Bey et al.,22 and Huang et al.23 either isolated the supraspinatus tendon, only added loads to the infraspinatus, or used loads much smaller than 22 newtons on the infraspinatus and subscapularis. The addition of increased loads on the infraspinatus and subscapularis could be a possible explanation for the higher strain values, which more accurately represent the physiologic loading conditions of the RC.
Based on our findings, we can conclude that strain increases with GH abduction angle, and the posterior region of the supraspinatus exhibits the largest strain. As it has been shown that RC tears will propagate towards the region with the highest strain,15 a better understanding of the mechanical environment could help predict tear progression characteristics. It has been long established that degenerative RC tears initiate in the anterior region of the supraspinatus tendon.40,53–55 However, a recent study has suggested that tears may initiate 13-17 mm posterior to the biceps tendon,56 which, according to traditional anatomical definitions, lies just anterior to the supraspinatus-infraspinatus junction.57,58 The findings from functional dynamic investigations indicate that partial supraspinatus tendon tears result in a biomechanical distortion and functional impairment comparable to that observed in cases with full-thickness tendon tears.59 We hypothesize that tears originating in the anterior region are more likely to propagate posteriorly due to the high strain within that region, and tears that originate in the posterior region are less likely to propagate, as the anterior region is mechanically stronger and experiences lower strains. Further studies identifying the region of tear initiation and, most importantly, where they most commonly propagate may aid in the clinical decision-making of which RC tears should be surgically corrected in the early stages of the disease to avoid progression.
This work represents a step towards improved musculoskeletal health and patient outcomes in shoulder pathology. In terms of the clinical aspect, our findings provide clinicians with a deeper understanding of the mechanical dynamics governing the supraspinatus tendon during GH abduction. This knowledge can aid in developing treatment plans tailored to the specific regional strain patterns we identified. Although debridement is commonly acknowledged as a reasonable treatment approach for lesions that affect less than 50% of the tendon thickness, there is a significant gap in the knowledge about the histological parameters that influence tear progression.60 For shoulder orthopedic surgeons, these studies offer valuable insights to modify surgical techniques, such as repair and reconstruction procedures, allowing for a more tailored approach that addresses the specific needs of each tendon region. This information can be used to optimize outcomes and minimize the risk of re-injury, ultimately improving patient outcomes.
4.1. Limitations
The limitations of this study include those shared with all cadaveric studies,61 including using dead tissue to simulate human motion, a static scapular position, and single lines of action for muscle activation. The RC muscle activation was assumed to be constant during motion, which is unlikely true in vivo. This allowed for a direct comparison between conditions and an evaluation of how the abduction degree altered the supraspinatus tendon’s surface strain. Furthermore, this cadaveric model is limited to the RC and omits the deltoid, which assists the supraspinatus in abduction. The supraspinatus is known to be most active during 0-30° of abduction, but in this study, the range of abduction examined was 60° to 90°. However, previous studies have shown that the supraspinatus remains active through the shoulder’s entire range of motion.62,63 Furthermore, Kim et al.41 measured strain of the supraspinatus tendon in-vivo during active abduction from 0° to 90° and reported increasing strain with increasing abduction angle, with the peak strain occurring at 90°. Lastly, this study uses a small sample size, only evaluating five specimens. However, this is a limitation shared with many cadaveric studies.61 Although the sample size is small, this study highlights the differences in the regional strain response of the supraspinatus tendon, suggesting that future studies should look at average tendon strain and all regional strain values.
5. Conclusion
The findings from this study provide a better understanding of the mechanical environment of the supraspinatus tendon by evaluating the difference in material response within its three morphological regions during abduction. The posterior region of the supraspinatus tendon experiences the highest strain. The segmental location of supraspinatus tears should be considered when evaluating its management, accounting for the risk of tear progression. Such insights hold promise in enhancing our ability to tailor clinical approaches and interventions for patients with supraspinatus tendon-related pathologies.
Declaration of Conflict of Interest
The authors do not have any potential conflicts of interest in the information and production of this manuscript.
Declaration of Funding
This work was supported by the Joe Fallon Research Fund and the Dr. Louis Meeks BIDMC Sports Medicine Trainee Research Fund at BIDMC Orthopaedic Surgery Department.
Declaration of Ethical Approval for Study
Our institution does not require ethical approval for cadaveric studies.
Declaration of Informed Consent
No information in the submitted manuscript can be used to identify patients.