


Introduction
Xylazine (street name “tranq”), a non-opioid sedative approved exclusively for veterinary use,1 is being mixed with illicit drugs at increasing frequency.2 First documented in Puerto Rico in the early 2000s,3,4 xylazine is now becoming increasingly prevalent as an adulterant in the illicit drug supply in the continental United States,5 especially in the northeast.1,5–7 Xylazine serves as an inexpensive additive for illicit drug manufacturers to reduce the amount of opioids required per dose. Drug users find the additive desirable as xylazine extends the length of the opioid high. In 2019, the Philadelphia Department of Public Health in Pennsylvania discovered a third of intravenous drug-related deaths involved xylazine exposure.2,5
Little is known about the long-term consequences of xylazine exposure, and there is limited research on the effects of xylazine when used in combination with opioids. When used in humans, xylazine can cause respiratory depression, hypotension, bradycardia, and central nervous system depression.5,8 When combined with opioids, there can be a synergistic effect leading to severe respiratory depression and increased risk of fatality. While the reversal agent naloxone plays a critical role in responding to opioid-related overdoses, naloxone is ineffective against xylazine, and there has not been a reversal agent yet identified in humans. Additionally, xylazine injection has been linked with unique skin ulcerations, predominantly on the extremities.3,4,9 These wounds worsen with ongoing xylazine use and can further progress to soft tissue infection and osteomyelitis.3,4,10
Patients presenting with large areas of xylazine-induced skin necrosis require a multidisciplinary approach with psychiatry/addiction medicine, orthopedic surgery, wound care, infectious disease, and plastic and reconstructive surgery. These wounds often require multiple debridements, wound care with dressings or negative pressure therapy, and soft tissue reconstruction. Reconstruction poses a unique and challenging scenario for the reconstructive surgeon as recurrent drug abuse can damage a successful reconstruction or create new areas of soft tissue necrosis requiring further reconstruction. The reconstructive surgeon can be challenged with how far to push reconstructive efforts in the setting of ongoing drug abuse, given the morbidity to the patient and the strain placed on healthcare resources. With the ongoing opioid epidemic, xylazine-laced opioids have become an increasing public health concern. In this paper, we present a case example of xylazine-induced skin necrosis and a treatment course to highlight the complexities and ethical considerations associated with the reconstruction of these wounds.
Case Report
A 38-year-old female with a past medical history significant for intravenous drug use, bipolar disorder, and anxiety initially presented to our wound care center with bilateral dorsal forearm wounds. She reported injecting approximately 20 bags of fentanyl a day, which were adulterated with xylazine. Surgical consultation for debridement was recommended; however, she was noncompliant with this recommendation. She performed daily dressing changes but continued to inject into the wounds and surrounding tissue daily.
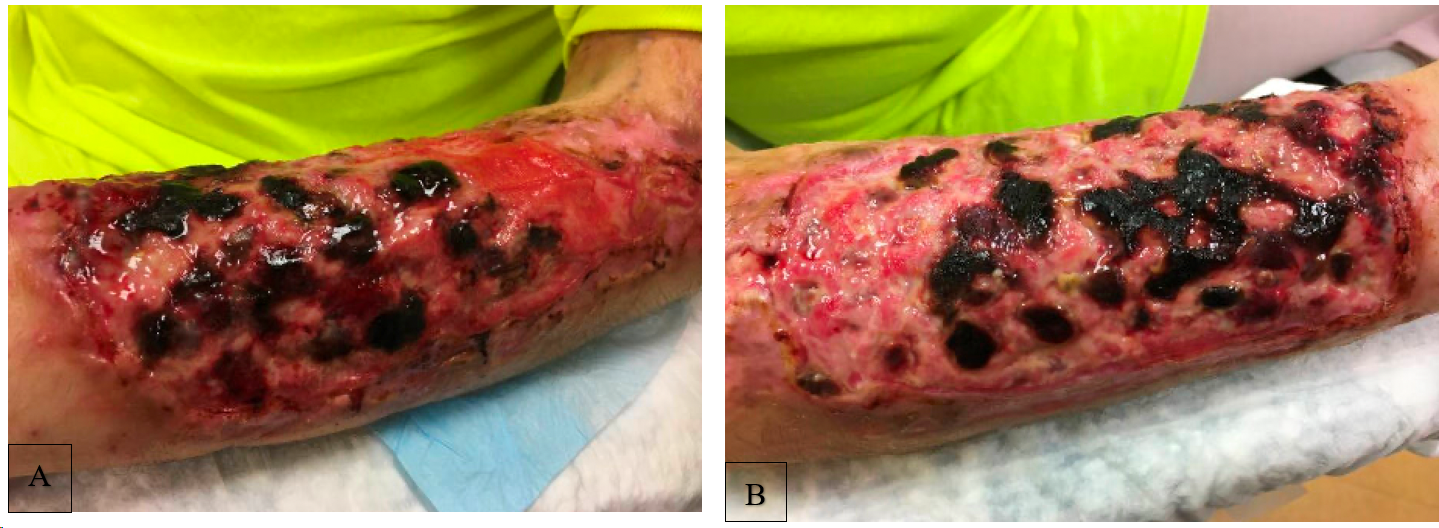
She ultimately re-presented six months later with concerns of a wound infection. On examination, she had large eschars on her bilateral dorsal forearms measuring 15x10 cm on the right and 10 x 12 cm on the left with surrounding cellulitis [Figure 1].
_left__(b)_right.png)
She had limited extension of her wrists bilaterally and numbness in the left superficial radial nerve distribution. Of note, she also had significant scarring in her antecubital fossas from previous drug injection-related wounds, resulting in flexion contractures of both elbows. She was admitted for intravenous antibiotics and was followed by both psychiatry and addiction medicine for the management of her addiction and withdrawal symptoms. She was taken to the operating room by orthopedic surgery for debridement, revealing full-thickness skin loss with exposure of left forearm extensor tendons, with paratenon intact. Cultures grew methicillin-resistant Staphylococcus aureus (MRSA), and she was treated with vancomycin. She underwent negative pressure therapy on her forearm wounds, and a plastic surgery consult was obtained. Reconstructive options were discussed, including nonoperative management with dressing changes or negative pressure wound therapy and operative management with split-thickness skin grafting. She elected for surgical reconstruction with skin grafting.
Prior to reconstruction, while undergoing negative pressure wound therapy, she left against medical advice (AMA) with negative pressure dressings in place; however, she was readmitted the subsequent day, expressing regret and asking for reconstruction. She was again evaluated by psychiatry and addiction medicine, and while she declined inpatient rehabilitation, she agreed to methadone treatment prior to reconstructive efforts. She underwent another week of negative pressure wound therapy in the hospital and did not try to leave AMA again. After many conversations with the patient and her healthcare teams, split-thickness skin grafting was pursued.
The patient underwent successful split-thickness skin grafting of both bilateral forearm wounds with a donor site from the left thigh. She remained inpatient with negative pressure therapy over the grafts. The negative pressure therapy was removed on post-operative day 5, and a complete take of the skin grafts was confirmed [Figure 2].
_left__(b)_right.png)
She was discharged with daily dressing changes. At the time of discharge, she was titrated on methadone and was connected to a methadone clinic to continue outpatient treatment. At one month post-operatively, her bilateral grafts were confirmed healed [Figure 3]. She was subsequently lost to follow-up.
_left__(b)_right.png)
The patient returned to the wound clinic approximately nine months postoperatively with complaints of new bilateral lower extremity necrotic wounds. She also confirmed that she had continued with her methadone treatment but had relapsed by supplementing with fentanyl injections. She was injecting into her legs to avoid her reconstructed forearms. The wounds were extensive, with significant necrotic tissue, foul odor, and surrounding cellulitis. Admission was recommended, and a few days later, she was taken to the operating room for debridement. Large full-thickness skin loss of her bilateral lower legs with extensive scarring and loss of normal anatomical planes were identified. The resultant wounds were 30 x 25 cm on the right and 28 x 24 cm on the left, with cultures ultimately growing Proteus species. She remained inpatient and underwent negative pressure therapy for two weeks prior to definitive reconstruction. During her hospitalization, she was followed by addiction medicine and expressed interest in sobriety but continued to refuse inpatient rehabilitation. She returned to the operating room and underwent split-thickness skin grafting to her bilateral lower extremities with donor sites from bilateral thighs. Still refusing inpatient drug treatment, she was discharged home with daily dressing changes.
Approximately one month following bilateral lower extremity reconstruction, the patient returned to the emergency department with new full-thickness bilateral forearm wounds with complete destruction of the previous soft tissue reconstruction. She had exposed denuded extensor tendons with a significantly diminished range of motion of wrist and fingers and absent dorsal hand sensation bilaterally. [Figure 4].

She was evaluated by orthopedic surgery and plastic surgery. Given the continued threat of any soft tissue reconstruction to ongoing drug use and the associated use of healthcare resources, an ethics consultation was obtained to discuss the ethical considerations surrounding any further reconstructive efforts. Ultimately, in discussion with orthopedic surgery, psychiatry, and ethics, it was felt that the benefit of reconstruction did not outweigh the risks unless her underlying addiction was appropriately addressed. As such, further reconstructive surgeries would only be offered if she was concomitantly receiving inpatient treatment for her addiction. As she adamantly refused inpatient rehabilitation, local wound care was recommended, and further reconstruction was not offered. She left AMA and has been lost to follow up since.
Discussion
Xylazine as an emerging adulterant in the opioid epidemic
On April 12, 2023, the Biden-Harris administration officially declared fentanyl adulterated or associated with xylazine as an emerging threat to the United States.11 While not Food and Drug Administration (FDA)-approved for human use,12 xylazine is being mixed with illicit fentanyl, heroin, and cocaine. In a recent study with data from all four United States (US) Census regions, xylazine is being increasingly detected in overdose deaths, with the highest prevalence in Philadelphia (26% of deaths), followed by Maryland (19%) and Connecticut (10%).13 Many drug users are unaware of the presence of xylazine in their drug supply.14 The motivation behind using xylazine as an adulterant is likely multifactorial. Firstly, it can be used as a bulking agent, allowing distributors to extend their drug supply.7 Secondly, xylazine is thought to enhance or prolong the effects of opioids.5,8,13
Studies show similar pharmacologic effects comparing xylazine and opioids in humans, including bradycardia, hypotension, central nervous system depression, and respiratory depression8,15,16; thus, synergistic effects may occur when used together. However, unlike opioids, naloxone cannot reverse the effects of xylazine. Along with its central depressive effects, xylazine also introduces a new public health dilemma for its profound skin necrosis effects, yielding complex reconstructive challenges. To date, there are limited reports in the literature of xylazine-related wounds.12,17 A recent report by Soderquist et al. identified severe limb compromise in 8 patients from Philadelphia warranting surgical intervention, including limb amputation.17
Pharmacokinetics of xylazine and mechanism of skin injury
Xylazine was first synthesized in 1962 by Bayer (Leverkusen, Germany) for use in veterinary analgesia and sedation.18 It is a partial alpha-2 adrenergic agonist with a chemical structure similar to dexmedetomidine, clonidine, phenothiazines, and tricyclic antidepressants.19 Binding of xylazine to alpha-2 receptors results in a decreased release of norepinephrine and dopamine, leading to sedation, muscle relaxation, and reduced perception of painful stimuli.20 Other alpha-2 adrenergic agonists are used in humans as adjuncts in anesthesia to reduce the requirement for general anesthesia. The pharmacokinetic parameters of xylazine are well understood in animals; however, little is known about its effects in humans. In animals, the drug is quickly distributed to the central nervous system, and its effects can last 30 minutes to 4 hours. Elimination half-life varies from 23-49 minutes.8
Like other alpha-2 agonists, Xylazine induces peripheral vasoconstriction by activating peripheral alpha-2 receptors.21 Peripheral vasoconstriction leads to tissue ischemia, skin necrosis, impaired wound healing, and infection.22 As painful wounds develop, users may continue to inject in the region to treat the associated pain, thus propagating the ischemia in the area and worsening wounds. Additionally, xylazine lowers cardiac output and thus lowers the delivery of oxygen to end organs, such as the integument. This would presumably increase the ischemic effect on the skin. However, further studies would be necessary to definitively determine xylazine’s effect on oxygenation of the integument and its association with wound formation.
Ethical considerations around reconstruction in adulterant-induced wounds
Medical ethics, a concept first introduced in 1803 by Thomas Percival, is based on four principles: respect for autonomy, beneficence, non-maleficence, and justice.23 These principles shape modern physician’s medical decision-making, especially in complex situations like the case report presented in this paper.
Autonomy describes a patient’s right to choice and freedom in their medical care. For this principle to be upheld, patients must be competent and able to understand a proposed treatment’s risk and benefit profile. The principle of beneficence describes the duty to provide benefit to a patient and remove potential harm where possible. The principle of non-maleficence describes the act of not intentionally causing harm to a patient through an action or failure to act. While this principle seems relatively straightforward, all medical decision-making has possible harms. The principle of justice is that each patient is entitled to their fair share of available resources. With this principle, providers balance healthcare goods and services for their patients while balancing the needs of others and society. These four principles serve as the foundation for decision-making; however, it is possible for two or more principles to conflict, thus offering unclear guidance in care.
Our case of recurrent xylazine-induced wounds exemplifies a difficult clinical scenario that is faced by people injecting drugs like fentanyl. In our patient’s case, the four ethical principles conflicted with one another and could not give clear guidance on a treatment pathway. Should the patient have been offered surgical reconstruction for her leg wounds after demonstrating an inability to abstain from drugs after her prior forearm reconstruction? Should surgical reconstruction have been offered for her recurrent arm wounds when she presented again with ulceration of the previous reconstruction? This ethical dilemma can be found in other clinical scenarios as well, including persistent intravenous drug use resulting in recurrent endocarditis requiring repeat cardiac surgeries and valve replacements.24 The American College of Cardiology and the American Heart Association guidelines recommend cardiac valve surgery whenever infected endocarditis arises, even after prior valve replacement.25 However, a 2019 study by Straw et al. reviewed patients with intravenous drug use with infected endocarditis requiring cardiac valve replacement, which still resulted in a 51% risk of recurrent infected endocarditis due to persistent intravenous drug abuse.26
Returning to our case of recurrent xylazine-induced wounds, the principle of autonomy would suggest that, given that she was found to have the capacity for decision-making, the patient has the right to choose her medical care, including reconstruction and drug rehabilitation. Refusing further reconstructive surgery if desired by the patient would violate autonomy. Additionally, the patient has the autonomy to choose whether she pursues drug rehabilitation; however, without rehabilitation, any reconstructive attempt will likely be obliterated with future xylazine use. Refusing further surgery would also be in violation of the principle of beneficence, as failing to reconstruct the wounds surgically could lead the patient to increased distress, increased risk of infection, and prolonged wound care and healing course.
However, surgery does not come without its risks. One can argue that ongoing surgical reconstruction would violate the principle of non-maleficence as continuing to harvest skin grafts from the patient could present undue harm to the patient. With recurrent large surface wounds, donor sites for grafting become limited and may need to expand to other parts of the body, causing more donor site morbidity. Additionally, with her ongoing drug use and subsequent destruction of the reconstructed sites, the benefit that the patient received from reconstructive surgery, if any, was very limited. Without drug rehabilitation, the underlying disease is not being treated, and soft tissue reconstruction is simply a band-aid for the symptoms. Given these considerations, the benefit/risk ratio for surgery decreases.
The last ethical principle to consider in our case scenario is justice, which indicates that resources for our patient should be balanced with resources for others. Each time our patient was admitted, she utilized significant resources, thus limiting the resources available to others. Each hospital stay was approximately three weeks or longer to allow for debridement, wound bed preparation, and skin grafting. The patient could not be discharged because of being unreliable for an outpatient follow-up. As such, she occupied a hospital bed and clinical resources when beds, nursing staff, and supplies were limited secondary to the COVID-19 pandemic. Additionally, she required multidisciplinary care, with providers from hospital medicine, infectious disease, psychiatry, addiction medicine, pain/palliative care, ethics, wound care, orthopedic surgery, and plastic surgery. In summary, while offering ongoing surgical intervention could support autonomy and beneficence, it could violate the principles of non-maleficence and justice.
As injected xylazine-adulterated fentanyl becomes an increasing threat, hospital systems and providers will be faced with this ethical conundrum more frequently. One possible option would be to provide medically necessary care (i.e., intravenous antibiotics if infected or debridement if necrotic tissue was found) but only offer definitive soft tissue reconstruction in the setting of inpatient rehabilitation for drug addiction. There is precedent across surgical specialties of withholding surgery until medical comorbidity that either increases the risk of surgery or jeopardizes the outcome is mitigated. For instance, surgeons require patients to quit nicotine prior to many elective surgeries as nicotine poses an unnecessary risk in the result of the surgery. Similarly, many transplant centers across the country require alcohol abstinence for six months prior to receiving a liver transplant.
If amenable, drug-addicted patients could be discharged to a drug rehabilitation facility that is equipped to provide daily wound care. Once the addiction is managed, soft tissue reconstruction with autograft, xenograft, or flaps can be pursued. With treatment of the underlying addition, the risk of ongoing damage to the reconstruction with drug use is minimized, and the longevity and benefit of the reconstruction are maximized. Ultimately, even if patients comply with preoperative requirements, there is still a risk of relapse, resulting in damage to the reconstruction. This is a risk that both the patient and the surgeon must be aware of and willing to assume. Some surgeons may adopt a “one and done” policy, offering one soft tissue reconstruction in the setting of adulterant or drug-induced wounds but no further reconstructions if the patient continues using drugs. If this approach is taken, a surgeon must be transparent with the patient prior to the first reconstruction.
Xylazine-adulterant poses a growing public health threat in the United States. As more patients present to hospitals after injection with xylazine-adulterated fentanyl, an increased understanding of the associated risks and complications of its use is required from specialties such as emergency medicine, addiction medicine, psychiatry, infectious disease, pain management/palliative care, ethics, orthopedic surgery, and plastic and reconstructive surgery. Our case example allows for a timely discussion of the ethical considerations for reconstruction in xylazine-induced skin necrosis. While there is no correct answer, and each patient needs to be considered as an individual, we hope to start the conversation on how to manage these difficult cases.
DECLARATION OF CONFLICT OF INTEREST
The authors do NOT have any potential conflicts of interest related to the content presented in this manuscript."
DECLARATION OF FUNDING
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
DECLARATION OF ETHICAL APPROVAL
The affiliated institution does not require ethical approval for reporting individual cases.
DECLARATION OF INFORMED CONSENT
There is no information (names, initials, hospital identification numbers, or photographs / images) in the submitted manuscript that can be used to identify patients. Informed consent to review, write up, and public this case was obtained from the patient.