
INTRODUCTION
The Achilles tendon is the most commonly injured, even though it is the largest and strongest.1 Recent research has revealed little difference in re-rupture rates in those treated nonoperatively vs. operatively.2 With sports being the most common cause for rupture of this tendon, it is important that the repair method is strong to reduce the risk. Some surgical options include the Krakow, Giftbox, Speedbridge, and Bunnell techniques.3 For college or professional athletes, in particular, surgical repair is typically the treatment of choice due to the improved functional gains and more predictable recovery timeline compared to nonsurgical patients.4
Despite this, there are several challenges with operative repair. These include wound infection, nerve damage, and re-rupture.4 These complications other than re-rupture have been reported as high as 34%.5 A review by Mansfield et al. reported that the return to play rate of athletes is consistently around 80%, with an average return to play time of 11 months in the literature.4 However, athletes typically can only return to preinjury performance levels 2-3 years out from surgery, with some athletes experiencing shortened athletic careers.4 This paper aims to describe a new surgical technique that adapts the modified giftbox.6
INDICATIONS & CONTRAINDICATIONS
There is little consensus on absolute indications and contraindications for surgical treatment of Achilles tendon ruptures. Some indications may include both acute (<6 weeks) and chronic (> 6 weeks) ruptures that are amenable to primary repair with a gap less than 5cm.7 Contraindications may include medical comorbidities that make the patient unfit for surgery, wounds, or ulcers near the planned incision, among others.
Patients who require higher demands of their Achilles tendon, like highly active individuals and athletes, will benefit from a surgical approach for the reasons discussed above.4 In contrast, older or less active individuals may not necessarily benefit from a surgical approach. The inherent risks of surgery may not be worth the potential gain in the older or less active individual. A nonoperative approach may be more optimal. The authors maintain that while there is no chronological age limit for this technique, we prefer that the patients indicated for open repair with the new modified giftbox are physiologically young, active individuals with well-controlled medical conditions and nonsmokers. Patients with diabetes or inflammatory arthritides on biologic medications are indicated on a case-by-case basis but with a preference that they are well-controlled in terms of their hemoglubin A1C and no active skin lesions at the site of the planned incision. We strongly recommend holding biologics and steroid medications until suture removal and adequate wound healing (approximately 2-3 weeks postoperatively).8 Lastly, for patients with chronic ruptures, we prefer to obtain an magnetic resonance imaging (MRI) preoperatively to investigate the proximal tendon retraction or gap distance, gastrocnemius-soleus muscle fatty atrophy, and to assess the integrity of flexor hallucis longus (FHL) muscle-tendon unit to plan for allograft reconstruction or salvage FHL tendon transfer instead of primary repair, respectively.
SURGICAL TECHNIQUE
Surgical Preparation
The surgeon’s preference is that the patient undergoes a popliteal and saphenous nerve block before being transported to the operating room. Anesthesia is induced via general endotracheal intubation or, less commonly Monitored Anesthesia Care (MAC) sedation then the patient is placed prone on the operating table [Figure 1-A]. A hip bump is placed under the ipsilateral hip to help with exposure. A thigh tourniquet is used and inflated to 275 mm Hg after exsanguination.
_operating_room_setup_with_the_patient_in_a_prone_position_ensuring_that_the_operative_l.png)
Surgical Equipment
The necessary surgical equipment for this modified giftbox technique includes a #2 Fiber Wire suture, a straight Keith needle, and a curved free needle. Self-retaining or Army-Navy retractors will aid in visualization.
Surgical Steps
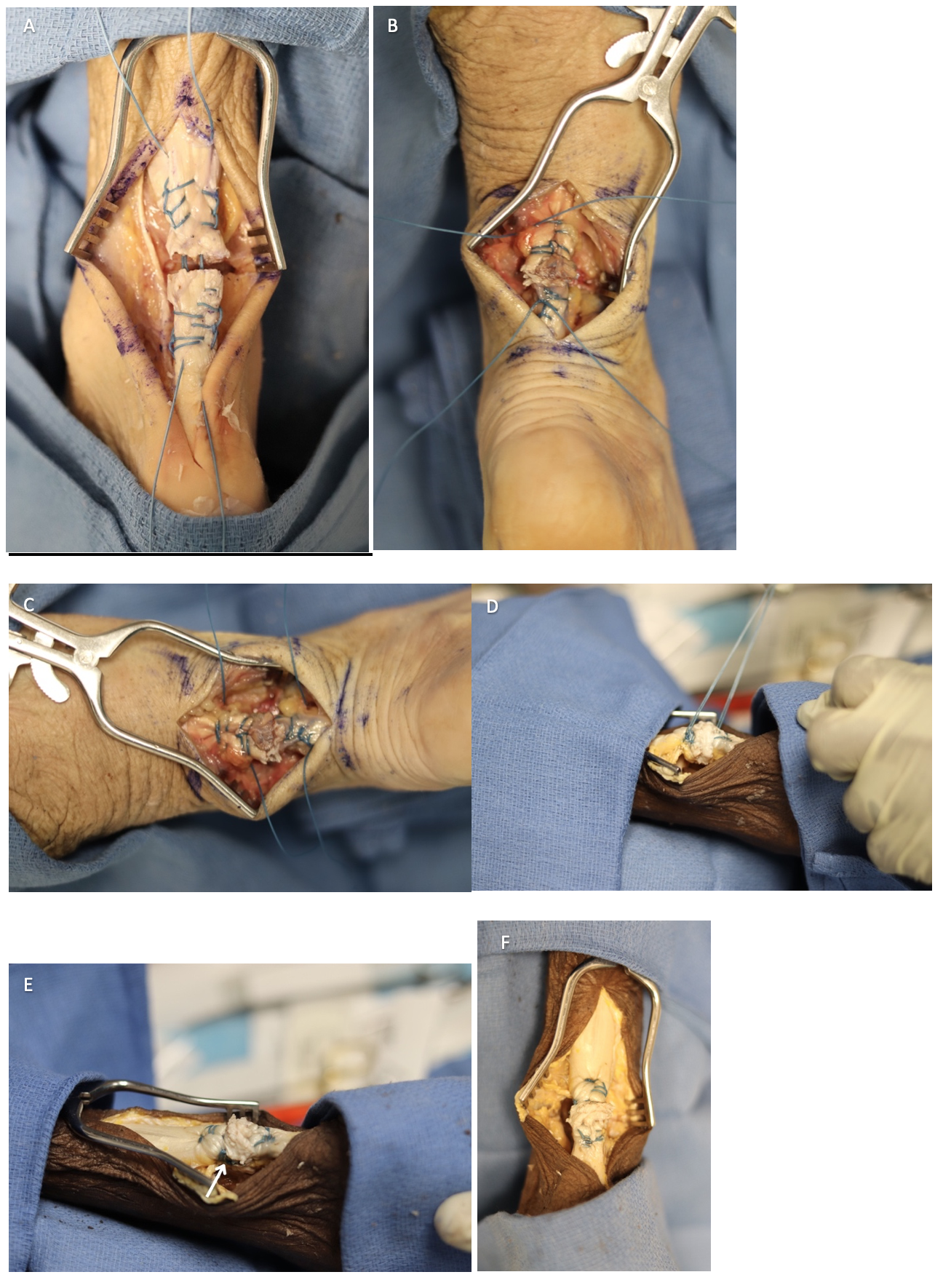
The revised Modified Giftbox technique used in this study is a novel technique created by one of the primary investigators (MVH) which builds on the original description by Labib.6 A paramedian approach to the Achilles tendon rupture is used, and a longitudinal incision about 5-6cm is centered at the rupture site [Figure 1-B]. The incision is carried down through the skin to the paratenon, and we avoid any blunt dissection or creation of tissue flaps until we split the paratenon layer in line with the incision. The technique involves the following: #2 Fiber Wire used to Krakow the proximal and distal limbs of the ruptured tendon, with all four suture ends exiting in the middle between both tendon ends [Figure 1-C and 1-D]. Next, a Keith needle is used to bring each limb of suture proximal and distal in a crisscrossed pattern (i.e., distal medial suture goes lateral and proximal within the tendon and vice versa). [Figure 2-A] Then, the two limbs of suture exiting medially and laterally are tied together for the proximal aspect and then repeated at the distal aspect of the repair, ensuring no gap at the rupture site and maintaining tension at all times [Figure 2-B]. Next, a free needle is used to bring each limb at the proximal aspect from superficial to deep (anterior to the tendon); this is repeated for the distal sutures. We now have two limbs of suture proximal and two limbs distally on the anterior surface of the tendon. Next, we tie the two lateral-based tails, proximal and distal, together to create a side strut. This is repeated on the medial aspect of the tendon, therefore fortifying our repair with a “belt and suspenders” repair [Figure 2-C and 2-D]. Care is taken to lay this suture knot on the anterior surface. Lastly, one suture limb from both the lateral and medial struts is tied together. The remaining suture tails are cut to create only one main suture mass on the anterior surface of the Achilles tendon [Figure 2-E]. Finally, ensure all knots are buried with no significant suture mass before closing the surgical wound [Figure 2-F]. The wound is copiously irrigated with saline and then closed in layers, ensuring a deep closure that re-approximates the paratenon and subcutaneous tissue over the repair.
_suture_tails_passed_more_proximally_and_distally_to_the_krakow_configuration_with_keit.png)
Post-Operative Management
Patients are placed in a short-leg plaster splint immediately postoperatively and then transitioned to a below-knee cast during their one-week postoperative clinic visit. They will not perform any range of motion exercises or physical therapy for the first two weeks. After two weeks, they will transition to walker boots with one one-inch heel lift that they can wear at all times except for hygiene or physical therapy. Patients will steadily decrease their heel lift throughout the therapy period. At this stage, therapy will include exercises such as range of motion only to a neutral position with the knee flexed and stationary bike with a brace on. Starting at four weeks, the patient may progress to weight bearing as tolerated in the walker boot. Also, an increase in ankle range of motion exercises to include inversion/eversion and passive ankle plantar flexion. At eight weeks, patients should progress to doing full passive and controlled eccentric exercises with some light resistance exercises with the knee bent. At three months, the patient can transition to normal shoes and start passively stretching the Achilles with controlled eccentrics. Closed-chain exercises can be begun, and straight-line running can be done at five months. Six months and onwards, more sport or activity-specific training may begin. This postoperative management is adapted across the foot and ankle section of our institution; however, the senior author prefers to transition the patients from the postoperative splint to a below-knee cast rather than a controlled ankle motion (CAM) boot at the first postoperative appointment.
Short Term Outcomes
At the time of publication, there are 13 patients with short-term outcomes data, which include Foot and Ankle Ability Measure, Activities of Daily Living (FAAM ADL), and Visual Analog Scores (VAS) [Table 1]. There was an average improvement of FAAM ADL score over 9.5 months in patients with available data (26.1 vs. 90.9). There was also a decrease in the VAS scores (4.8 vs. 1.0). The overall complication rate was 30.8%, including one re-rupture, two infections and one instance of delayed wound healing.
DISCUSSION
Despite no universally accepted technique for Achilles tendon repair, end-to-end repair is widely used. The Krakow technique is common, and the giftbox technique has been shown to be stronger than the Krakow technique.6 Frantz et al. introduced their modified giftbox techniques in 2018.8 They provided good results with low complication rates.9 Our revised and modified giftbox technique differs from Frantz et al. and any other giftbox technique in that it has the benefit of (1) tying lateral and medial suture struts and (2) the final suture knot stack is anterior to the tendon, which may provide additional strength and less superficial skin irritation/pressure from the knots.3,9
Open primary repair is routinely used even though percutaneous techniques have become more common.10 However, there is an additional cost to such techniques, which may be more cost-prohibitive in certain reimbursement models. Open repair is also routinely used, especially in chronic rupture with retraction or pseudo-tendon formation. We believe that our revision to the Modified Giftbox will allow for fortifying the primary repair in those cases. However, future studies are needed to test our hypothesis.
This revised Modified Giftbox technique has potential risks, including nerve damage, poor wound healing, damage to other structures, thromboembolic events, etc.3 In addition to the previously stated pearls and pitfalls [Table 2], it is important to note that the surgeon must counsel their patients on the risks of surgical versus nonsurgical management of Achilles tendon ruptures. Generally, surgical treatment has been shown to have an increased risk of complications other than re-rupture.2 These risks should be discussed in a shared decision-making process between surgeon and patient, based on the patient’s risk tolerance and goals.
Limitations of this suture technique include suture bulk, especially in patients with low body habitus. However, this technique seeks to bury most of the suture mass anterior/deep to the Achilles tendon to avoid this complication. Additionally, some patients have been known to have inflammatory reactions to nonabsorbable braided sutures such as FiberWireTM; therefore, close monitoring of the incision and surrounding soft tissue within the postoperative period is imperative to identify patients who may have this suture-type reaction. Future studies will explore the short and long-term patient-reported outcomes of this surgical technique compared to others. In addition, a biomechanical study to evaluate the tensile strength of this technique is currently being conducted to compare it to other suture techniques.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
This study received the Institutional Review Board (STUDY20020136) and Committee for Oversight of Research and Clinical Training Involving Decedents approval for the use of photographs.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs / images) in the submitted manuscript that can be used to identify patients.