Introduction
Avascular necrosis (AVN) is inadequate vascular perfusion to a specific bone, resulting in degeneration of osteocytes and bone marrow that can progress to subchondral collapse.1 There are approximately 10,000 - 20,000 new cases of femoral head AVN reported in the United States annually.2 This can be correlated to several factors such as trauma, chronic alcohol or steroid use, autoimmune diseases, and coagulopathies like sickle cell disease.2 AVN is a rare complication resulting from an intraarticular corticosteroid injection, an intervention commonly used to address hip pain.3 Previous studies have compared the occurrence of femoral head AVN and subchondral collapse between patients who received a single corticosteroid injection and controls; no significant difference was found, with a very low rate in both groups.3,4 Thus, the risk of significant progression of joint degeneration is not often considered when using corticosteroid injections to address hip pain.
This case report presents a patient who developed AVN and subchondral collapse of the femoral head following a single intra-articular corticosteroid injection. To date, there have been few similar cases reported in the literature.
Case Report
A 51-year-old female with obesity, hypertension, and smoking history presented with progressively worsening right hip pain for the past year. The patient described the pain as dull and achy, becoming sharp at times, worsened with activity, and improved with rest. She received a previous trochanteric corticosteroid injection that did not alleviate her lateral hip or groin pain. She reported no chronic steroid use or bleeding problems. On the initial visit physical exam, the patient had a nonantalgic gait and pain with resisted hip flexion. She had a positive anterior impingement and a negative Patrick exam. Both special tests were negative in the left hip.
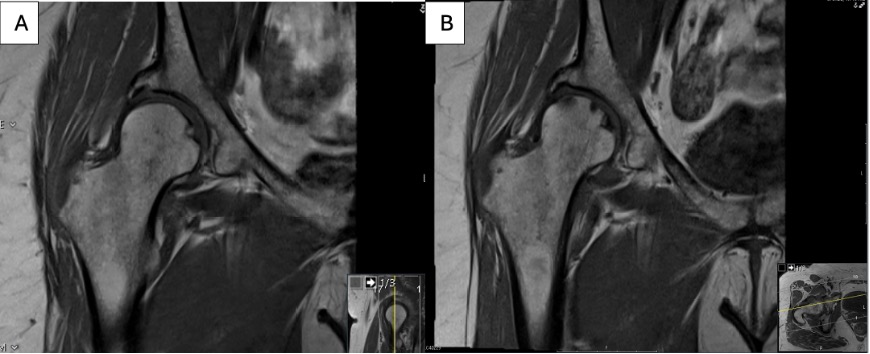
X-rays of the right hip obtained at the initial appointment showed evidence of osteoarthritis and significant hip dysplasia. A Magnetic Resonance Image (MRI) of the pelvis and right hip was obtained before the injection, showing osteoarthritic changes with no noted AVN, subchondral collapse, or insufficiency fracture [Figure 1].
The patient opted to receive an intraarticular corticosteroid injection in the right hip joint. Utilizing ultrasound guidance, an injection of 2cc of 1% lidocaine, 2cc of 0.25% bupivacaine, and 40 mg Kenalog was performed.
Four months following the injection, the patient presented with worsened pain after 2-3 months of initial pain relief. The discomfort was mild and localized to the greater trochanteric region. On physical exam, there was no visible swelling or deformity of the right hip, and no paresthesia was reported. A slight limitation to the active range of motion was noted due to pain, while muscle strength was comparable to the contralateral side. Mild discomfort was noted with the logroll. At this visit, the patient elected to move forward with a second corticosteroid injection; however, aspiration of the joint prior to injection revealed 2-3 mL of straight heme. Thus, the procedure was discontinued, and the patient was scheduled for an MRI to rule out possible AVN and subchondral insufficiency fracture/collapse. The repeat MRI showed evidence of secondary AVN and mild subchondral collapse that had significantly progressed since the previous MRI [Figure 1].
__showing_osteoarthritic_changes_wi.jpg)
Due to potential sequelae from additional corticosteroid injections, particularly the progression of AVN and further subchondral collapse, the patient decided not to receive another injection. Given the patient progressed into AVN and subchondral collapse, failing to adequately respond to nonoperative treatments such as Non-steroidal anti-inflammatory drugs (NSAIDs) and activity modification, they subsequently elected to undergo a total hip arthroplasty.
Discussion
Avascular necrosis is a lack of sufficient perfusion to a bone that leads to severe degeneration and is most prevalent in the femoral head. AVN of the femoral head is most commonly correlated to trauma, but it has also been described most often in association with chronic steroid and alcohol use.2 AVN is a rare complication of an intraarticular corticosteroid injection; the first case was reported by Yamamoto et al. in 2006, involving a 50-year-old female who developed femoral head AVN three months post-injection.5 To our knowledge, seven similar cases have been published before this report [Table 1].5–10
All reported patients have been in the 5th-7th decades of life and received a single corticosteroid injection to treat hip osteoarthritis. All patients reported worsened hip pain after some level of temporary relief from the injection, and AVN was demonstrated between 4- and 18 weeks post-injection. Some cases, such as those in Ahmed et al., involved patients who had medical histories that may have increased their risk: 1) post-traumatic osteoarthritis from a previous fracture-dislocation that was surgically repaired two years prior and 2) psoriasis with ongoing modulated immunotherapy treatment.6 The patient in this report exhibited none of the aforementioned risk factors; there was no history of excessive alcohol or steroid use, bleeding problems, or trauma to the hip. Also, unlike the one described in this report, not all cases included pre-injection MRI scans to rule out preexisting AVN.6,7,9,10
MRI is important in the diagnosis of AVN and ruling out other potential diagnoses like rapidly progressive osteoarthritis. Early-stage AVN appears as serpentine-shaped areas of edema that progress to diffuse areas with foci of necrosis in later stages. Still, rapidly progressive osteoarthritis exhibits characteristic linear areas of edema parallel to the articular surface.7 Septic joint caused by injection is another potential diagnosis; however, given this patient’s timeline, history, and physical exam, such a differential is less likely. Infection, however, should be ruled out through the history, physical exam, laboratory workup, and possible joint aspiration with fluid laboratory analysis.
AVN can be managed nonoperatively by limiting weight-bearing and pharmacological therapies, often with limited success. Operative options include joint-preserving surgeries when no subchondral collapse is present, such as bone decompression, autologous bone marrow transplant, and bone grafting. However, arthroplasty is indicated once AVN has progressed to subchondral collapse.10
While rare, AVN should be considered as a possible complication from the administration of intraarticular corticosteroid injections in the hip and a high suspicion of AVN in patients with risk factors and/or rebound pain should be maintained. Early recognition of warning signs, such as worsened pain or disability 1 to 4 months after injection, especially following a temporary period of improvement in symptoms, is essential to help prevent rapid joint deterioration and the need for replacement. Providers should counsel patients on these warning signs at the time of injection and encourage follow-up immediately if any of these symptoms arise. If a patient presents with rebound symptoms or opts to receive a second injection and heme is aspirated from the joint, an MRI should immediately be ordered with a high suspicion of AVN. Quickly diagnosing AVN and initiating conservative treatment or intervening with joint-preserving surgery may help prevent this complication from resulting in THA.
Conclusions
Hip pain that worsens or reappears in the first 1 to 4 months after administering an intraarticular corticosteroid injection may indicate a need for further evaluation to rule out the development of avascular necrosis of the femoral head. Early recognition may help prevent the rapid progression of AVN to subchondral collapse, requiring arthroplasty, as demonstrated in this patient. This emphasizes the importance of close patient monitoring and follow-up after an intraarticular corticosteroid hip injection
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support in the preparation, research, authorship and publication of this manuscript.
Declaration of ethical approval for study
The IRB at this institution does not require approval for case reports.
Declaration of informed consent
There is no identifiable information in this manuscript