
INTRODUCTION
Carpal tunnel syndrome (CTS) is the most common peripheral entrapment neuropathy, estimated to affect up to 5% of the total population.1 CTS is caused by median nerve compression and is caused to be primarily idiopathic but can occur secondarily from conditions such as diabetes, hypothyroidism, and pregnancy. When nonoperative treatments fail, the surgical release of the transverse carpal ligament (TCL) is a reliable treatment option.2,3
Carpal tunnel release (CTR) surgery can utilize both an open and endoscopic approach. Open carpal tunnel release (OCTR) is the traditional method of carpal tunnel release, where direct visualization of the TCL is achieved prior to transecting. Common complications following OCTR include continued weakness, pillar pain, and increased scarring at the surgical site.4 Endoscopic carpal tunnel release (ECTR) was first reported by Okutsu et al. and Chow et al. in 1989, providing an alternative method of CTR.5 A 2020 meta-analysis of 28 randomized control trials concluded that the endoscopic approach has greater patient satisfaction rates and pinch strength, decreased scarring, and a faster return to work time.6 However, many studies suggest that long-term outcomes, including symptom relief and complications, do not differ between open and endoscopic approaches.7–9
Despite the proposed benefits of endoscopic surgery, the current literature suggests that the open approach is still preferred.10,11 However, the modality of carpal tunnel surgery remains a highly debated topic, with multiple studies reporting supporting evidence for both techniques. This study aims to quantify the utilization of open and endoscopic CTR in the United States (U.S.) over ten years to better understand how the orthopedic community responds to the literature on this topic. The study hypothesis is that the utilization of endoscopic CTR has been increasing. Based on our study’s epidemiological findings, we anticipate our results will complement the existing research on indications, costs, and outcomes for open and endoscopic CTR. This collective knowledge can facilitate more comprehensive and informed decision-making in patient surgical selection.
METHODS
About the TriNetX network
The TriNetX database was retrospectively queried in March 2024 for patients 18 to 90 years old with CTR surgery from January 1st, 2014, to December 31st, 2023. The TriNetX database does not involve patient-identifiable information and is subsequently exempt from Institutional Review Board review and approval. The TriNetX U.S. Collaborative Network is a large, de-identified research network encompassing data from more than 60 U.S. health care with more than 100 million patients. It contains de-identified aggregate patient information covering procedures, diagnoses, medications, vitals, genomics, and demographics. Healthcare Organizations (HCOs) involved in the TriNetX network contribute healthcare data in de-identified, pseudo-anonymized, or limited dataset formats, following local privacy regulations. These HCOs are authorized to use this data on the TriNetX platform for research purposes. In return for providing data, HCOs incur no financial expenses and gain access to data query tools, analytics, visualization capabilities, and the necessary hardware for software execution. The de-identification process conforms to Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule standards, as verified by a qualified expert, meeting the requirements of Section §164.514(b)(1), ensuring HIPAA compliance.
TriNetX Data Extraction
Patients with current procedural terminology (CPT) codes for open (cpt 64721) or endoscopic (cpt 29848) CTR surgery between 2014 and 2023 were identified. Baseline characteristics, including age, sex, race, and body mass index (BMI), were collected. Total CTR (open and endoscopic) rates were calculated as a ratio of CTR out of total carpal tunnel syndrome diagnoses per year. Utilization of each surgical approach was calculated using a proportion of open-to-endoscopic CTR each year from 2014-2023. Ten-year data for open, endoscopic, and total surgeries were collected and separated by region, including Northeast, Midwest, South, and West [Figure 1].

RESULTS
A total of 215,115 patients were identified as having CTR from 2014-2023, including 169,917 open and 45,198 endoscopic releases. Mean age (± Standard Deviation (SD)) was 64 (±15) for the open and 63 (±14) for the endoscopic cohort. Most patients were female, making up 58% and 61% of the OCTR and ECTR cohorts, respectively. Both cohorts were predominantly white (71% in the open and 78% in endoscopic). Body mass index (BMI) (± SD) was 31.2 (±7.0) for open and 31.7 (±7.0) for endoscopic release [Table 1].
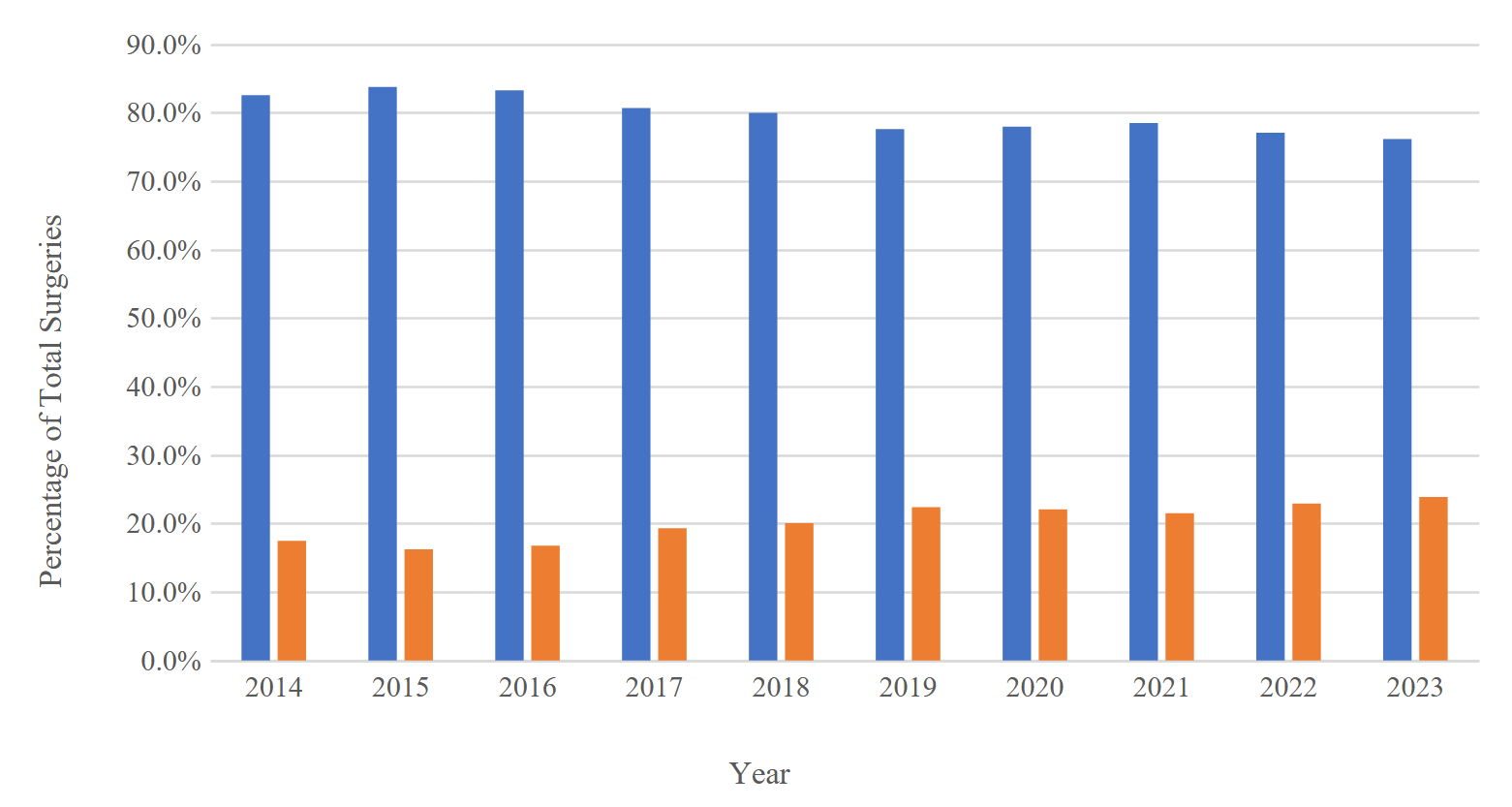
Overall total, open, and endoscopic CTR surgery rates have increased over the last decade. Rates of total surgeries increased from 10.5% in 2014 to 15.4% in 2023 [Table 2, Figure 2]. In 2014, open surgery accounted for 82.5% of total CTR surgeries, while endoscopic surgeries accounted for 17.5%. Over the ten years, the proportion of endoscopic surgery increased from 17.5% in 2014 to 23.9% in 2023 [Table 2, Figure 3].


Overall, the South had the greatest utilization of endoscopic surgery, with 32.2% of CTR from 2014-2023 being endoscopic. Endoscopic surgeries accounted for 18.9% of total CTR in the Northeast. The West (11.1%) and the Midwest (10.6%) were regions with the least endoscopic usage [Table 3].
DISCUSSION
The study results suggest that both open and endoscopic CTR rates are increasing, which correlates with prior epidemiological studies.12,13 Burton et al. demonstrated increasing rates of CTR in the UK up until 2007, with subsequent tapering rates14 and Roquelare et al. showed a decreased incidence of CTR in France.15 In a UK study, hand surgery referrals have increased by over 36%, with CTS being the most common diagnosis for hand surgery referrals.16 The increased rate of diagnosis and surgical treatment is likely related to greater awareness of the diagnosis and improved understanding of its surgical outcomes.
It is known that CTS disproportionately affects females more commonly than males.17–19 This study’s results show a similar predilection for female CTR patients. A recent study by Carroll et al. identified a surgical cohort that was 62% and 61% female for open and endoscopic CTR, respectively. This study identified rates of 58% for open and 61% for endoscopic CT, which mirror these findings. There were no demographic differences between the two cohorts in this study, similar to Carroll et al.'s study.20
At the time of this study, it has been 35 years since Okutsu et al. first introduced the endoscopic approach for CTR in 1989.5 Numerous studies have demonstrated accelerated rehabilitation and a quicker return to work for the endoscopic approach.21–23 However, this study confirms that open CTR is still the predominant technique for CTR. Yet, while OCTR remains the predominant technique, this study’s results show an overall increase in the proportion of ECTR to OCTR each year. A 2017 Medicare study mirrored this study’s results with a 5% growth rate for ECTR compared to 0.9% for OCTR over seven years.24 This may be partially attributed to the increase in hand-fellowship trained surgeons,25 as utilization of endoscopic CTR is higher among these surgeons.26 Furthermore, increasing patient preference,27 purported benefits of decreased scar tenderness and increased pinch strength,28 and lower costs of endoscopic CTR with higher reimbursement rates24 may be contributing to increasing endoscopic utilization. Future studies that can quantify the annual numbers of surgeons involved in CTR may help further clarify if increased hand-fellowship-trained surgeons are the cause of increased ECTR utilization.
The Southern U.S. region was found to have the greatest utilization of ECTR. This may be partially attributed to findings from a 2018 study where the geographic distribution of hand specialists in the U.S. was analyzed. In the US, 38% of all hand surgeons were found to reside in the South, with the Northeast, Midwest, and West making up 22%, 21%, and 19% of hand surgeons, respectively.29 Smetana et al. found that hand-fellowship trained surgeons have higher utilization of the ECTR technique,26 thus making intuitive sense that regions with higher proportions of hand specialists exhibit greater rates of its utilization. However, Rios-Diaz et al. noted inequities in hand surgeon distribution in the U.S., with increased fellowships and subspecialists in higher per capita income regions, particularly on the Northeast and West coasts. This study somewhat refutes this hypothesis; thus, further investigation of regional variations in ECTR utilization is needed.30
When interpreting the findings of the study, certain limitations should be considered. First, the retrospective cohort design of the TriNetX database is inherently limited and relies on complete and accurate data entry. Furthermore, a proportion of our population contained unknown data regarding sex and race, preventing the determination of exact demographic values. Rates of CTR may also have been overestimated compared to the general population. Patients with a documented diagnosis of CTS are likely to have more severe symptoms necessitating medical care and potentially surgery compared to patients who do not seek medical care for milder CTS symptoms. Additionally, improvements in patient documentation over the last decade, leading to more accurate and comprehensive charting, may have influenced the observed trends in utilizing OCTR and ECTR.
CONCLUSION
CTS is the most common peripheral neuropathy, and the usage of surgical management for the condition continues to rise. From 2014-2023, the rates of both open and endoscopic CTR in the U.S. have increased, with the open technique being used more frequently. However, the proportion of endoscopic CTR surgeries has steadily increased over the last ten years and has not plateaued as of 2023. Additionally, the study identified the South as the region in the U.S. with the greatest utilization of the endoscopic approach.
DECLARATION OF CONFLICTS OF INTEREST
The authors do NOT have any potential conflicts of interest in the information and production of this manuscript.
DECLARATION OF FUNDING
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
DECLARATION OF ETHICAL APPROVAL
This study using the TriNetX database does not require IRB approval.
DECLARATION OF INFORMED CONSENT
No identifiable patient information is present within the manuscript.