
Introduction
Minimally Invasive Plate Osteosynthesis (MIPO) has been a widely accepted and, in certain instances, the superior method of fixation when it comes to various long bone fractures, with benefits ranging from fracture stability and early mobilization to accelerated fracture healing secondary to the preservation of periosteal blood supply. Such stability effectively reduces pain, facilitates functional recovery, and ultimately promotes accelerated recovery compared to conventional open surgical techniques.1–4 Various MIPO techniques have been described to maintain the blood supply to the comminuted fracture fragments and to accelerate bone healing.1,5–7
The current state-of-the-art techniques utilize external fixators or distraction devices to allow for adequate alignment and maintenance of fracture reduction. Devices range from K-wire distractors and single-sided half-pin frames Arbeitsgemeinschaft für Osteosynthesefragen/Association for the Study of Internal Fixation (AO/ASIF) to specially designed tibial reduction devices such as the Staffordshire Tibial Orthopedic Reduction Machine (STORM).8,9 Nonetheless, these procedures have been associated with extended surgical time, increased infection risk, and prolonged pain and discomfort, with additional morbidities.10,11 Manual distraction requires extra staff to hold the reduction, potentially adding to the cost and time.6,12–14 The reduction quality depends on the consistency and fatigue of the manual traction, risking over-distraction of the fracture.
Ligamentotaxis is a principle of fracture reduction in which the fractured bone fragments are aligned with the assistance of the surrounding soft tissues, muscles, and ligaments under tension. Unlike reductions via direct manipulation or external devices, ligamentotaxis indirectly reduces the fracture by utilizing the natural vector forces of surrounding structures.15 The fracture reduction method described in this study leverages the principle of ligamentotaxis by positioning the patient in a supine position on a conventional operating table, with the affected leg hanging down the edge of the bed, allowing gravity-induced traction.
Surgical Technique
Our study included patients with fractures classified as 41-A2, 41-A3, 42B, and 42C according to the AO Foundation and Orthopedic Trauma Association classification (AO-OTA). Exclusion criteria included open tibial fractures, tibial fractures associated with neurovascular injury, and displaced intra-articular plateau fractures. All surgeries were performed by a single surgeon on a regular operating table. After obtaining informed consent and institutional ethical review committee approval, we included three patients with extra-articular comminuted proximal tibial fractures.
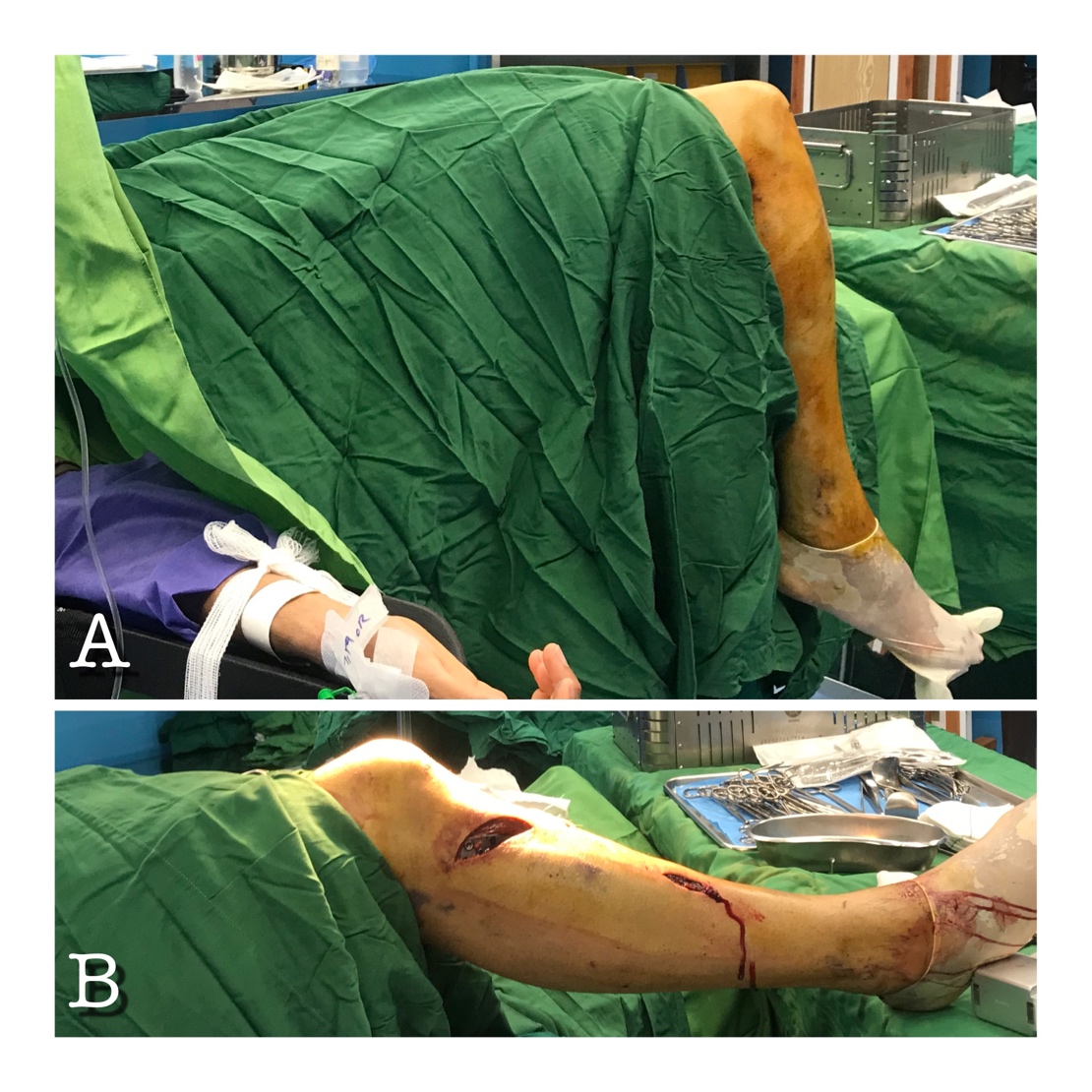
The patient is placed in the supine position on a conventional operating table with a thigh tourniquet. A bolster was placed under the knee to put the hip in 10 to 15 degrees of flexion and 30 to 40 degrees of abduction to facilitate limb positioning. The leg was then hung from the distal edge of the bed, allowing optimal access and visualization of the fracture site while preventing forward flexion of the fracture. In the hanging position, the knee rests in 90° to 95° of flexion due to gravity. This positioning allows for seamless adjustment of the knee joint, enabling it to be easily flexed from full extension of 0° to 60° as needed during the procedure, thereby facilitating optimal surgical access and maneuverability [Figure 1A].
_and_after_(b)_fixation.jpeg)
The contralateral extremity was positioned in a leg holder with both the hip and knee flexed to approximately 30 degrees and hip abduction to achieve a hemi-lithotomy position. This allowed the surgeon unobstructed access to the affected area while enabling the precise placement of the C-arm in a horizontal orientation for obtaining clear lateral radiographs.
Following anesthesia and muscle relaxation, the first traction phase was carried out using the gravity force for about five minutes to elongate the muscles further and restore the bone length. Further, ligamentotaxis and manipulation can achieve reduction without any additional traction devices. The gravity reduction can be checked under fluoroscopy
A limited anterolateral proximal tibial approach was then performed, followed by an anatomical proximal lateral tibial locking plate placement. Two proximal locking screws were placed to stabilize the plate and prevent rotation, followed by two distal cortical screws placed through a minimal incision under fluoroscopic guidance [Figure 1B]. After confirming appropriate reduction and alignment under fluoroscopy, additional locking screws were inserted [Figure 2].

Partial weight bearing was started using crutches on postop day 1, followed by progressive weight bearing and full weight bearing by postop week six. Compression wrapping was used for the first 6 weeks, and patients received aspirin 81 mg twice daily for 6 weeks. Physical therapy started at postop week two.
The mean surgical time was 35 ± 8 minutes. All surgeries were done by a single orthopedic surgeon and one scrub nurse. All patients were followed up for 2 to 3 years with no reported intraoperative or postoperative complications, returning to low-demanding work in less than 14 days. All patients reached complete bone union in less than 24 weeks using the RAST score, evaluated by two independent reviewers. A list of pearls and pitfalls of gravity-based minimal invasive plate osteosynthesis for proximal tibia fractures are presented in [Table 1].
Discussion
The technique of close reduction in minimally invasive osteosynthesis of comminuted proximal tibial fractures has conventionally depended on distraction devices and external fixators for fracture reduction.16 While these methods have been widely adopted, they are associated with notable limitations, including increased operative time, higher infection risk, and significant patient discomfort.10,11 External fixators, such as the AO/ASIF half-pin frames and specialized devices like the Staffordshire Tibial Orthopedic Reduction Machine (STORM), play an essential role in fracture alignment but come with some drawbacks. Studies have shown that external fixation devices are prone to complications such as pin tract infections, soft tissue damage, and prolonged recovery times.6,8,13 Additionally, the cost and availability of external fixators pose significant challenges, particularly in resource-limited settings. The average price per external fixation frame, approximately $5,900, further emphasizes the need for more accessible alternatives.17 These factors, combined with the technical demands of these devices, create barriers to optimal fracture management and patient outcomes.
Minimally Invasive Plate Osteosynthesis (MIPO) has gained popularity in recent years as a preferred method for managing proximal tibial fractures, mainly due to its minimally invasive nature and preservation of periosteal blood supply. MIPO allows for early mobilization and faster recovery, reducing the risks of infection and soft tissue damage often seen with more invasive procedures.1,3,5,18
Seyhan et al. described a positioning technique for intramedullary nailing of closed tibial fractures that utilizes manual traction and gravity to assist with fracture reduction.19 Their technique, which avoids the need for specialized traction equipment, is beneficial in achieving accurate fracture alignment in closed fractures. However, their findings revealed limitations when applying this method to comminuted proximal tibial fractures, where intramedullary nailing often resulted in malalignment and hardware failure. These findings are consistent with other literature suggesting intramedullary nailing is not ideal for comminuted proximal tibia fractures due to the complexity of maintaining fragment alignment. For these challenging fractures, MIPO emerges as a more reliable alternative.19
Kim et al.'s study further supports this notion by demonstrating that MIPO, particularly when combined with careful soft tissue management, is highly effective for both open and comminuted proximal tibial fractures.5 The study followed patients with various fracture types, including complex, comminuted fractures, and found that MIPO offered excellent clinical outcomes with low rates of malalignment and infection, especially when primary MIPO was used. Their results showed that when soft tissue coverage is sufficient, MIPO allows for precise reduction and stabilization without exacerbating damage to already compromised areas. This directly relates to the manuscript’s exploration of gravity-based MIPO techniques, as both methods emphasize minimizing trauma to the soft tissues while achieving reliable fracture reduction and alignment.
Similarly, Van Nguyen et al.'s study on distal tibial fractures provides evidence of MIPO’s advantages, particularly for complex fractures.18 In their prospective case series, MIPO effectively managed complex and comminuted fractures with excellent union rates and minimal complications. The use of medial locking plates and indirect reduction techniques enabled patients to return to function earlier than traditional fixation methods. The study highlighted that MIPO not only reduces soft tissue injury but also minimizes the risk of malunion, which is particularly important in comminuted fractures where maintaining alignment can be challenging.
These studies underline the significance of MIPO as a superior option for managing complex and comminuted fractures of the tibia. The gravity-based reduction technique described in the manuscript builds upon these established principles, offering a novel method that enhances the MIPO procedure by using gravity-induced ligamentotaxis for reduction. The gravity-based technique simplifies the reduction process, reduces operative time, and decreases the risk of soft tissue complications by minimizing the need for manual traction or external fixation devices. It is particularly suited for comminuted fractures where traditional methods like intramedullary nailing may fail.
Our main limitations were the small sample size and limited access to the contralateral limb in polytrauma patients and obese patients. Future studies with larger sample sizes and various body habitus would be beneficial in further solidifying gravity-based minimal invasive plate osteosynthesis as a proximal tibial fracture reduction method.
In conclusion, our gravity-based MIPO technique offers a novel, economically viable solution to the limitations of conventional methods. By eliminating the need for external fixators and reducing operative complexity, this method holds significant promise for improving both clinical outcomes and cost-effectiveness, particularly in resource-limited settings. Further studies with larger sample sizes and long-term follow-up are needed to validate the safety and effectiveness of this approach entirely.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
The local ethics committee has waived this case series study.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.