Introduction
The proximal radioulnar joint (PRUJ) is the articulation between the radial head and the lesser sigmoid notch of the ulna.1,2 The PRUJ, the distal radioulnar joint (DRUJ), and the interosseous ligament (IOL) form an integrated osseoligamentous system that allows forearm rotation and distributes applied forces.3 The radial head is a key stabilizer to axial load and valgus stress at the PRUJ. When radial head fractures cannot be managed with open reduction and internal fixation, radial head arthroplasty is often indicated. Proper radial head prosthesis sizing is critical since “overstuffing” the radiocapitellar joint alters kinematics, increases joint pressures, and may lead to degenerative changes, pain, and weakness.4–7 Overstuffing occurs if the prosthesis is larger than the native radial head.
Several studies have investigated elbow anatomy to improve understanding and potentially inform optimal prosthesis sizing and design. Shin et al. conducted a computed tomography (CT) study to examine pressures and stresses on the radial head and coronoid articular surfaces.8 Their findings contribute valuable insights that may aid in the design of prostheses, though the study did not specifically propose a method for determining appropriate prosthesis sizing. Doornberg et al. identified radiographic landmarks on CT for optimal radial head prosthesis insertion.9 These reference points may also guide algorithms for selecting properly sized implants, although no definitive guidelines exist beyond matching the excised radial head. Sun et al. proposed that measuring the lateral capitellar diameter on preoperative CT scans could help predict the optimal size for a radial head implant.10 CT imaging, however, cannot assess cartilage thickness and involves additional cost and radiation exposure compared to standard radiography.11–13 Currently, the prosthesis size is determined using the resected head’s diameter and length and the ulnohumeral joint’s congruity as a guide. The chosen prosthesis is checked clinically against the sigmoid notch and radiographically to ensure the ulnohumeral joint is not gapped open by overstuffing.
Previous radiographic studies on radial head prosthesis positioning do not fully address the anatomic variance of the PRUJ.14,15 We define “PRUJ variance” as the distance from the equator of the radial head projection to the proximal-most portion of the coronoid process. Literature on using plain radiographs to determine PRUJ variance for optimizing prosthesis sizing is sparse. Building on Doornberg et al.'s work, we aim to assess plain radiographs as a safer, more cost-effective alternative to CT for evaluating PRUJ measurements. We hypothesize that plain radiographs can offer valuable data on PRUJ variance, improving radial head prosthesis sizing and potentially enhancing patient outcomes after arthroplasty.
Methods
After approval from the institutional review board, we retrospectively reviewed consecutive elbow radiographs at a tertiary care trauma center. Inclusion criteria required all radiographs be performed on patients over 18 years of age, with adequate radiographs available for review. Anterior-posterior (AP) radiographs were used with the elbow in full extension and supination. This position was chosen as it is the standard projection performed in elbow imaging and is the position of maximum PRUJ congruity, as described by Kim et al.14 Due to the variability in technique for the lateral projections resulting in heterogeneous images in our sample and the inability to adequately assess overstuffing, the lateral radiographs could not be used for evaluation. Patients who had a fracture or dislocation from the humeral shaft to the distal radius were excluded from the study to eliminate the contribution of the distal humerus or interosseous membrane to PRUJ positioning. Patients were also excluded if an Essex-Lopresti injury was suspected, identified radiographically as a radial head fracture with misalignment of the radius and ulna, or clinically by tenderness at the DRUJ in addition to the proximal radius. This exclusion was necessary because the compromised integrity of the IOL could lead to measurement inaccuracies at the PRUJ.
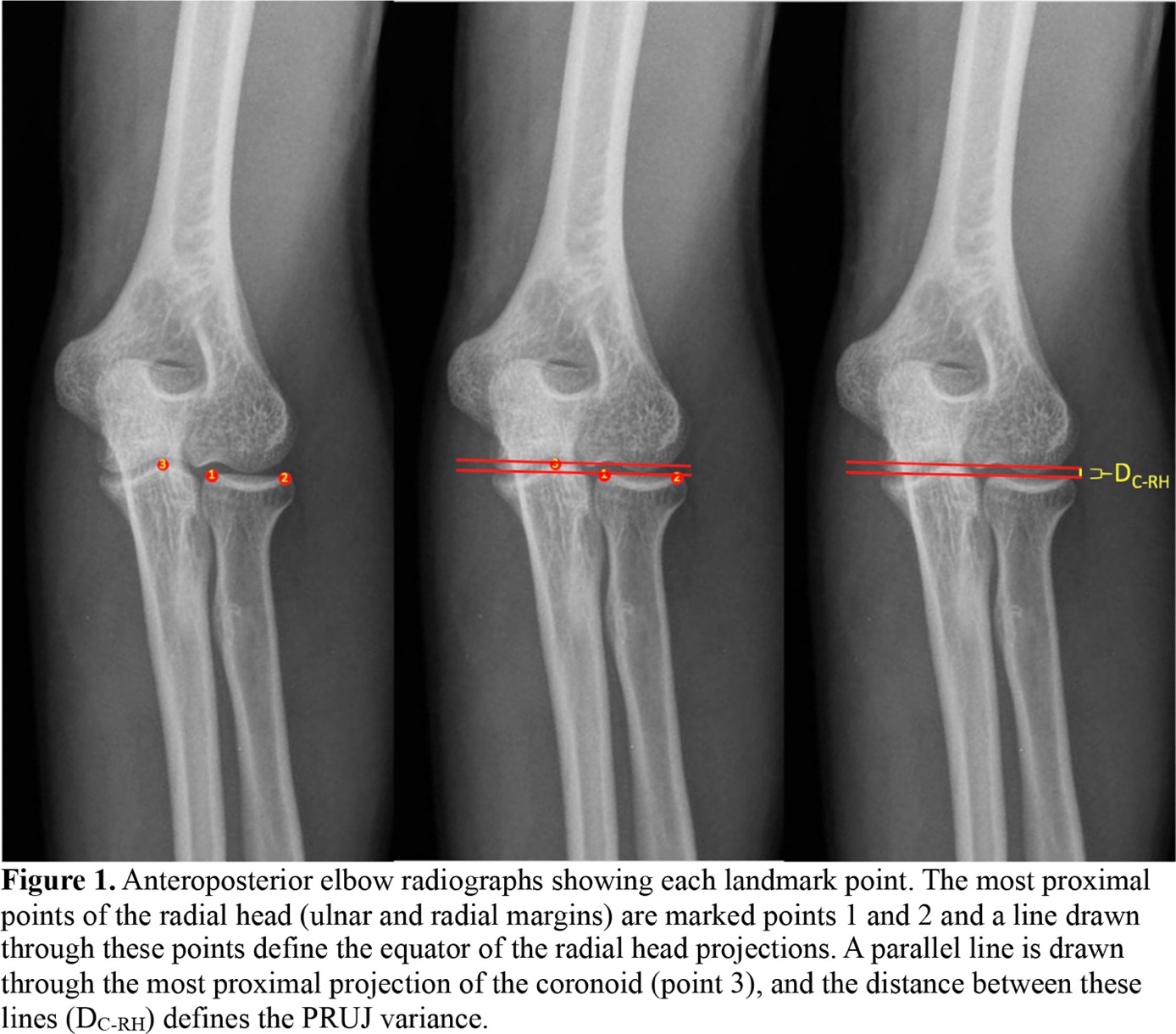
Elbow radiographs from one year at our institution were sequentially reviewed until fifty radiographs met the inclusion criteria. Upon chart review, the indication for radiography, age, sex, height, weight, and body mass index (BMI) were recorded. One fellowship-trained orthopaedic hand surgery attending, one senior orthopaedic surgery resident, and one junior resident assessed the radiographs for a measure of PRUJ variance. The radial head reference point was chosen as the equator of the radial head projection, drawn from the most proximal radial rim of the radius to the most proximal ulnar rim. The measurement performed was the anteroposterior (AP) coronoid to radial head height, defined as the distance from the equator of the radial head projection to the most proximal coronoid projection [Figure 1]. The proximal coronoid projection was selected as a landmark because it is consistently identifiable on standard AP X-rays, uniquely reflects each patient’s anatomy, and is a reliable reference point for guiding implant size based on our experience. All measurements were performed through the digital picture archiving and communication system (PACS, Boston, MA). Data was analyzed to determine measures of central tendency using Microsoft Excel (Seattle, WA) for average PRUJ variance. Interobserver reliability was analyzed using SPSS Statistics Software (Armonk, NY).

Results
Three reviewers reviewed fifty radiographs of atraumatic elbows. There were 37 males (74%) and 13 females (26%) in this cohort. The mean age of the patients was 40 years. With respect to laterality, 27 (54%) of the images were of the left elbow, and 23 (46%) were of the right. The average height of the sample population was 172.5 cm, with an average BMI of 28.6. The most common etiology was trauma, which was present in 16 (32%) of patients [Table 1].
When evaluating the measurements, the mean coronoid to radial head height was 2.2 mm, ranging from -2.6 to 5.2. For observer 1, a post-graduate year (PGY) 3 orthopaedic resident, coronoid to radial head height measurements ranged from -2.6 to 4.9mm, with an average of 2.3mm and a standard deviation of 1.6mm [Table 2]. For observer 2, a PGY 5 orthopaedic resident, coronoid to radial head height ranged from -2 to 5.2mm with an average of 2.3mm and a standard deviation of 1.5mm. For observer 3, a fellowship-trained hand and microvascular orthopaedic surgery attending, measurements ranged from -1.7 to 5.1mm with an average of 2.2mm and a standard deviation of 1.5mm. PRUJ variance based on patient height was investigated as a potential confounder by investigating the coronoid to radial height as a function of the patient’s overall height. No correlation was noted between PRUJ variance and height, with an R-squared value of <0.01. The inter-observer reliability was 0.95 (P<0.01) for the radial head to coronoid height.
Discussion
The PRUJ is the articulation between the radial head and the lesser sigmoid notch of the ulna. Due to the ovoid shape of the radial head and varying ligamentous tension with forearm rotation, the PRUJ shifts during pronation and supination.1,2,16–18 Proper positioning of the radial head during arthroplasty is critical because “overstuffing” the PRUJ can alter kinematics and joint pressures, leading to degenerative changes.4,6,7 Previous studies have used CT imaging to assess PRUJ variation and provide reference points—such as the posterior humeral cortex and coronoid process—for optimal radial head arthroplasty.8,9,19 However, reference points derived from standard radiographs remain limited. Preoperative baseline radiographs could guide intraoperative comparisons, potentially aiding in optimal radial head sizing. Moreover, examining a patient’s contralateral elbow may help tailor the implant to individualized anatomy.
Using plain radiographs, we found that while the percentage variation in PRUJ measurements was moderate, absolute variation was slight, supporting previous CT-based findings.9 Doornberg et al. reported a mean coronoid to radial head distance of 0.8 mm, indicating a slightly more distal radial head position relative to the coronoid, with a standard deviation of less than 1 mm.9 Our data align with this minimal absolute variance.
This limited variance in PRUJ contrasts with the DRUJ, which exhibits a broader range of ulnar variance.20 Inaccurate radial head sizing leads to undesirable changes in PRUJ variance, potentially causing degenerative changes, pain, and weakness due to altered kinematics and contact pressures at the radiocapitellar joint.4–7
From a safety perspective, radiation exposure is a concern. Sun et al. suggested that the lateral capitellar diameter measured on preoperative CT scans could predict the optimal radial head implant size.10 However, the use of CT scans raises considerations about radiation exposure. An extremity radiograph imparts about 0.1 mrem, while a CT scan of the extremity delivers approximately 10 mrem—a 100-fold increase.21 Although the risks from a single CT are low, reducing cumulative radiation exposure is prudent.22–26 This study suggests that plain radiographs can yield results comparable to CT in measuring PRUJ variance. Thus, radiographs may offer a suitable, lower-risk alternative to CT for evaluating radial head sizing during arthroplasty. A direct comparison between X-ray and CT assessments could clarify any subtle differences.
Cost considerations also favor radiographs. Medicare reimbursement for radiologist review of a two-view elbow radiograph is around $27.19, while that for an upper extremity CT is $168.56—more than six times higher.27 Facility fees further widen this gap, with elbow radiographs at about $540 compared to $1500 for CT scans. This disparity suggests potential cost containment if radiographs provide adequate anatomical detail.
A key strength of this study is the high interobserver reliability (0.95) achieved by observers with varying experience levels, from a junior resident to a fellowship-trained surgeon. Such consistency indicates that PRUJ measurements on radiographs can be widely applied, independent of training level. These results are comparable to those of Doornberg et al., who reported interobserver reliability values of 0.91 and 0.79 for coronoid height and lateral edge measurements, respectively.9 Another strength is that standard elbow radiographs obtained in full supination and AP projection can be used directly without special positioning instructions. Additionally, unlike CT scans, plain radiographs are readily available intraoperatively, allowing for dynamic assessment during surgery.
Several limitations merit consideration. First, we only evaluated AP radiographs in supination, not accounting for the radial head’s translation during the full rotational arc. Minor positioning changes could not be captured in two-dimensional images. To mitigate this, we included only optimal AP views, verified by all researchers. Optimal AP radiographs were ensured by examining for clear joint spaces between the humerus, radius, and ulna without any overlap, clearly visualized medial and lateral epicondyles of the humerus, and minimal overlap between the radial head and ulna, allowing clear visibility. Second, plain radiographs cannot measure cartilage thickness. Kim et al. found an average radial head cartilage thickness of 1.3 ± 0.4 mm, and differences in cartilage or osteophytes may influence PRUJ variance.14 This could be relevant in patients with osteoarthritis or other conditions not examined here. Third, our sample was predominantly male, possibly limiting generalizability. Fourth, while plain radiographs may help identify overstuffing or over-lengthening, contralateral comparisons are needed to confirm these findings. Using the opposite elbow as a control is reliable in many anatomical assessments, but we did not evaluate it in this study.28–30 Fifth, we assessed interobserver reliability but not intra-observer reliability, as each researcher measured only once. Finally, though our interobserver reliability was high, the number of observers was small, warranting further research to confirm these findings across broader groups.
Despite these limitations, we believe measuring the AP radial head to coronoid distance on standard radiographs is a reliable and practical method to assess PRUJ anatomy. This approach may offer a safer, more cost-effective alternative to CT imaging, providing valuable data for surgeons to optimize radial head prosthesis sizing and potentially improve patient outcomes.
Conclusion
Orthopaedic practitioners may prefer the presented measurement method because it is easily reproducible and attainable intraoperatively. The radiographic measures correlate with previously described CT findings and allow for a similar analysis of elbow anatomy without the radiation exposure and cost associated with a CT scan. As prior research has suggested the clinical use of CT imaging in appropriate preoperative planning, we provide evidence of a safer, more affordable evaluation method. These radiographic parameters can be used in the preoperative planning or intraoperative evaluation of radial head arthroplasties to assess optimal sizing and avoid overstuffing. Future investigation in the form of prospective studies with surgeons utilizing the described technique is warranted.
Declaration of conflict of interest
Author Michael M. Vosbikian, M.D. receives honorarium as section head of The Journal of Bone and Joint Surgery Clinical Classroom – Hand and Wrist, and honorarium for teaching pre-fellows course for Medartis. Dr. Vosbikian is an editorial board member for ePlasty and SurgiColl. The authors do not have any other potential conflicts of interest with respect to this manuscript.
Declaration of funding
The authors received NO financial support in the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
Institutional Review Board approval was received from Rutgers New Jersey Medical School (Study Number Pro20170000549)
Declaration of informed consent
There is no identifiable information in this manuscript