
INTRODUCTION
Hip fractures are a significant concern in the elderly population, with incidence rates increasing in recent years.1 The Center for Disease Control (CDC) reports that around 300,000 older adults are hospitalized annually for hip fractures.2 These fractures occur when the proximal femur breaks, often due to low-energy falls from standing height. Older adults are particularly susceptible due to age-related bone density loss, which accelerates after age 50.3 These injuries are both debilitating and costly, with estimated annual costs ranging from $10.3 billion to $15.2 billion.4,5 A patient can spend approximately $40,000 in the first year post-fracture and $5,000 in subsequent years.6 Optimizing patient outcomes is a critical study area given the increasing frequency and cost burden of hip fractures.
Pain control during the perioperative period is a crucial modifiable factor that influences patient outcomes following a hip fracture. High pain levels can hinder physical therapy, prolong hospital stays, and delay mobility.7 Poor perioperative pain management is also linked to increased post-operative delirium and complications,8 which further impede rehabilitation.9 Several options exist for pain management, including systemic analgesics, NSAIDs, opioids, regional anesthesia, and peripheral nerve blocks.4 Although opioids are commonly used for orthopedic pain control, their slower metabolism in older adults can lead to post-operative delirium and delayed recovery.10 This has spurred interest in regional forms of analgesia.
The Fascia iliaca block (FIB), a peripheral nerve block targeting the lateral cutaneous, femoral, and obturator nerves, has improved outcomes in elderly patients undergoing hip surgery.4,11–13 Studies demonstrate that pre-operative FIB lowers pain scores, reduces opioid use and postoperative delirium, shortens hospital stays, and decreases healthcare costs.11–19
Despite these benefits, FIB use is not universally applied. At our institution, it is included in the Geriatric Hip Fracture Protocol (GHFP), but the frequency of its administration remains uncertain. This study aims to evaluate the prevalence of FIB use upon admission for elderly hip fracture patients to improve timely administration. We hypothesize that most of these patients will not have received FIB before admission. While we found only one article assessing the frequency of FIB use following the implementation of a GHFP, our research offers a more longitudinal perspective, as our protocol has been in place for several years. We believe this study will benefit our institution and provide valuable insights for others in assessing the frequency of FIB use and addressing barriers that may hinder patient care.
METHODS
Study Design
This IRB #29515-approved retrospective chart review study examined the frequency of elderly patients with hip fractures who received a fascia iliaca block upon admission. Study participants were included based on inclusion and exclusion criteria determined by the investigators. The inclusions consisted of all patients, 60-89 years old, who presented to Temple University Hospital between January 1, 2019, and December 31st, 2021, with proximal femur fractures, as these patients are eligible to receive FIB per our protocol. Patients were excluded if they suffered from a periprosthetic fracture and if they suffered other traumatic injuries at the time of the hip fracture, including but not limited to the head, back, chest, or abdominal trauma, as these conditions could influence the decisions to perform a FIB. We included 248 patients in this study.
Data Collection
Patient information remained confidential by creating patient identifications for each patient. Data was then collected by looking at patient records. Variables that were collected included age, gender, race, height, weight, body mass index (BMI), comorbidities such as dementia, use of blood thinning medications, chronic kidney disease (CKD), intravenous drug use (IVDU), smoking history, and conditions involving the brain, heart, or lungs, date/time of presentation to the emergency department (ED), type of fracture, preoperative delirium, the primary team admitted to, whether a fascia iliaca block was performed, whether the team that performed the block was ED or anesthesia, fascia iliaca block amount, was there proper documentation of the block procedure, date/time of surgery, time to surgery from when they arrived in the ED, type of surgery performed, type of anesthesia (spinal vs general), whether there was postoperative delirium, and time to resolution of postoperative delirium.
Geriatric Hip Fracture Guidelines and Fascia Iliaca Block Procedure
The patient is triaged in the ED to receive immediate assessment and treatment. X-rays are obtained in the ED to confirm the presence of a hip fracture. After confirmation, analgesics are given to the patient. The ED physician notifies orthopedics and internal medicine to see the patient within an hour. Surgical consent is obtained for an orthopedic procedure where the orthopedic team will inform the operating room (OR) of the patient and the case. Depending on the patient’s criteria, the patient is then admitted to either internal medicine, orthopedics, or trauma. Fascia iliaca block procedure is done by anesthesiology acute pain services or ED physician to reduce pre-operative pain.
Statistical Analysis
All data was collected on an encrypted Excel sheet that was compliant with Health Insurance Portability And Accountability Act (HIPAA) guidelines. The de-identified data was sent to statisticians. The statisticians then used Statistical Package for Social Sciences (SPSS) software to analyze the data.
RESULTS
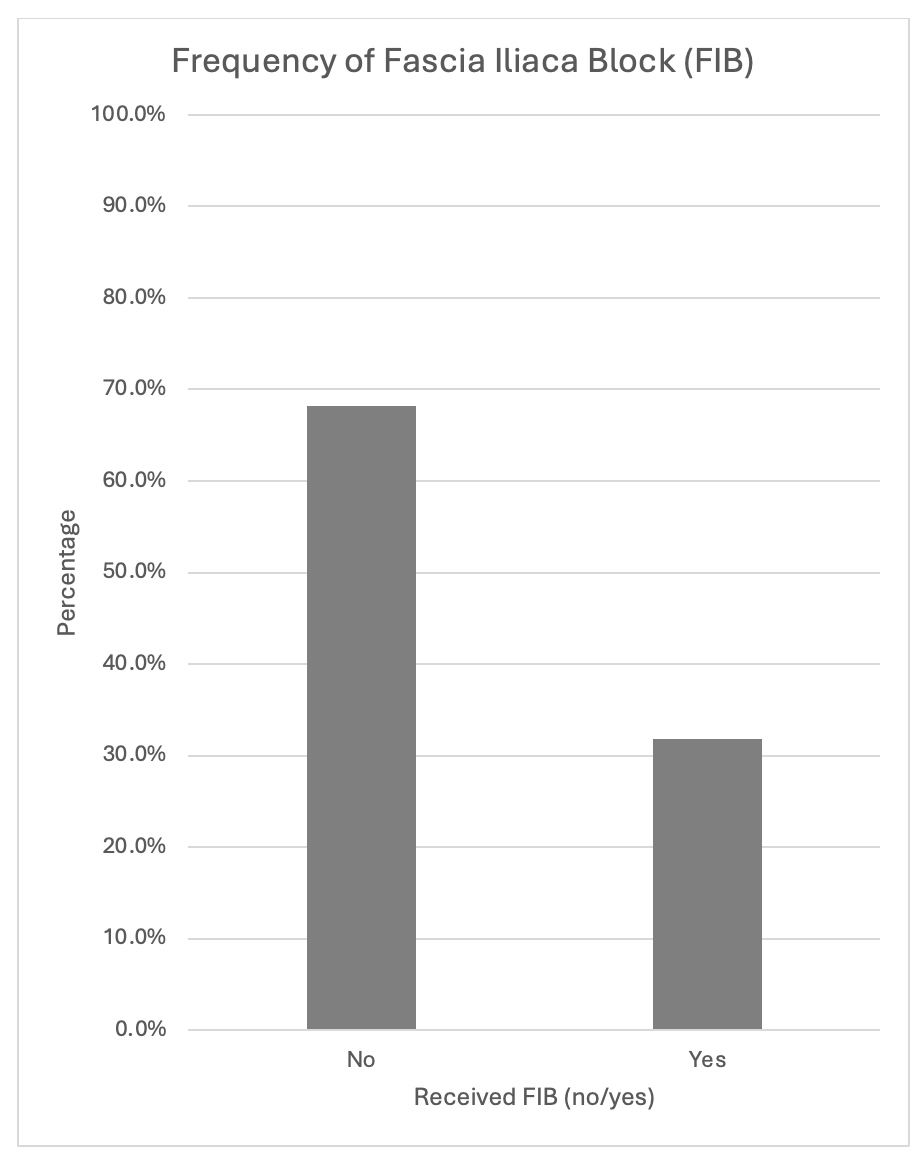
A total of 248 patient charts were reviewed for the study. The frequency and percentage of patients who received a FIB prior to admission and the characteristics of those who did and did not receive the block are summarized [Table 1].
Among elderly patients with hip fractures, only one-third (n = 79, 32%) received a FIB before admission, while the majority (n=169, 68%) did not [Figure 1]. Among those who received a FIB, the vast majority of procedures were performed by ED compared to anesthesia (95% vs 5.1%, p <0.001) [Figure 2]. All documented FIBs were appropriately recorded.


DISCUSSION
Despite abundant research demonstrating the beneficial use of FIBs,14–16 this retrospective chart review showed that most elderly patients with hip fractures at our institute are not receiving an FIB before surgery. Among the elderly patients who received the FIB, approximately 95% of them received the block while in the emergency department. Only 5% of these patients received a FIB from anesthesia following discharge from the emergency department prior to surgery.
Currently, no clear explanation exists for the low rate of FIBs being performed in elderly patients with hip fractures at Temple Hospital despite the procedure being a part of our geriatric hip fracture protocol. Studies have demonstrated that FIB is a relatively safe procedure. However, complications such as local anesthetic toxicity, nerve damage, infection, allergies, and bleeding are possible but rare in about 0.4% of procedures.20–22 Contraindications include previous femoral bypass surgery, patient refusal, allergy to local anesthetic, and infection at the block site.21 As effective pain management is critical for patients with hip fractures, NSAIDs and opioids can provide some benefits when FIB is not performed.4 However, the drawback to these is NSAIDs are more beneficial solely for mild pain management, whereas opioids can lead to post-operative delirium and delayed recovery in elderly patients.10 This evidence leads to research showing that FIB is a better alternative to improve outcomes in elderly patients undergoing hip surgery.4,11–13
One possible explanation for the low FIB rate is the shortage of trained emergency medical staff certified to perform an FIB. A lack of trained staff is one of the more frequent reasons why FIBs are not widely used.21 Not all emergency medicine physicians at Temple Hospital are certified to perform FIBs, meaning elderly patients with fractures must present to the emergency department when a certified physician is available. Additionally, there are time-dependent variations in when pain management and emergency medicine are expected to perform FIBs. Pain management is responsible for performing FIBs from 7 a.m. to 7 p.m., while emergency medicine covers the procedure from 7 p.m. to 7 a.m. Further research into these variables may clarify the low utilization rate of FIBs being performed at our institute.
The strengths of this study include a comprehensive chart review of patients who both did and did not receive FIBs. We minimized information bias by utilizing our institute’s standardized and easily accessible form for reporting FIB that was performed. However, the study’s limitations include reliance on non-structured data for delirium assessment, a small sample size, limited information in patient charts, and generalizability outside of a Level 1 trauma center.
The next step in this research is to address the concerningly low frequency of FIBs performed for elderly patients with hip fractures and to identify variables contributing to this. Determining why FIBs are not performed more frequently before surgery could help adjust protocols to ensure patients receive appropriate care. Our research provides a longitudinal perspective of having a GHFP in place that may be broadened to other institutions in assessing their own protocols and considering what barriers may be in place that hinder patient care in receiving FIB.
CONCLUSION
Our retrospective chart review revealed that the majority of elderly patients with hip fractures at our institute do not receive an FIB before surgery. These findings highlight a critical opportunity for quality improvement in pain management strategies to enhance outcomes for elderly hip fracture patients. Additionally, our experience can serve as a model for other institutions seeking to improve their perioperative care protocols for this vulnerable population.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
The authors received IRB #29515-approval for this study.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.