INTRODUCTIN
Distal humerus fractures (DHF) are increasingly common in the elderly population, largely due to the growing incidence of osteoporosis and increasing life expectancies. These fractures are often comminuted and intra-articular, presenting potentially complex treatment challenges, particularly in the setting of osteoporosis. By 2030, DHFs are expected to account for approximately 6% of all fractures in the elderly population.1 Given the constrained anatomy of the distal humerus and the functional demands of the elbow joint, nonoperative management is often insufficient. Historically, open reduction and internal fixation (ORIF) has long been considered the standard surgical treatment; however, in elderly patients with poor bone quality, this technique can be associated with fixation failure, prolonged immobilization, extensive rehabilitation, contractures, and suboptimal outcomes. Alternatively, total elbow arthroplasty (TEA) has emerged as an increasingly favored alternative for managing DHFs in the elderly population.2–4 Conservative approaches, such as the “bag of bones” technique, are often associated with suboptimal functional recovery and are now reserved mainly for nonoperative candidates.5
Previous studies, including early retrospective comparisons, have suggested that TEA may offer superior functional outcomes and lower complication rates compared to ORIF in elderly patients with complex DHFs.6 However, the landscape of TEA has evolved with newer implant designs, refined surgical techniques, and patient selection criteria that may affect outcomes. Despite this, there remains a relative lack of pooled data specifically evaluating modern TEA outcomes in acute trauma populations, highlighting the need for an updated synthesis of the evidence. The objective of this systematic review and meta-analysis is to evaluate the functional outcomes, complication rates, and implant usage trends of total elbow arthroplasty for acute distal humerus fractures using the most recent literature. By synthesizing data about functional scores and complication rates from contemporary studies, this review aims to inform clinical decision-making and clarify the role of TEA in the modern management of complex distal humeral fractures.
METHODS
Search Strategy
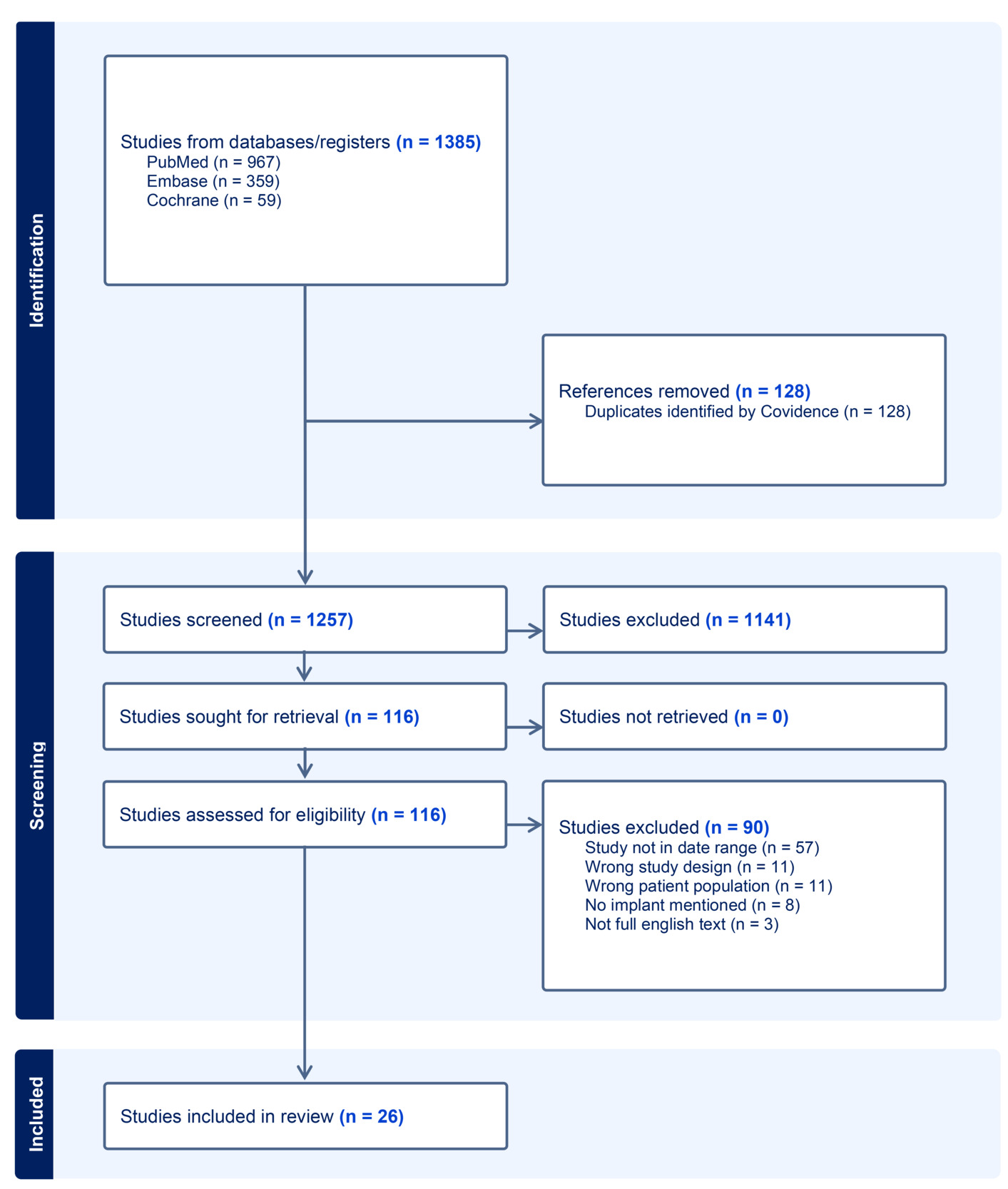
This systematic review was conducted using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol was registered with International Prospective Register of Systematic Reviews (PROSPERO) (CRD420251035898). A comprehensive literature search was performed across PubMed, Embase, and Cochrane Library databases through April 30, 2025. The search strategy incorporated both Medical Subject Headings (MeSH) and free-text keywords related to TEA, distal humerus fractures, and treatment outcomes. The full search string is provided in Supplementary Material 1. All identified records (n=1385) were imported into Covidence for screening and de-duplication. The reference lists of included studies were also manually reviewed to identify any additional eligible studies.
Eligibility Criteria
Studies were eligible for inclusion if they reported outcomes of primary TEA performed for acute distal humerus fractures, were published in English, and included original clinical data. This study also required each paper to have at least a three-month follow-up, as most complications occur by 30 days post-operatively. Additional inclusion criteria were a minimum of five adult patients (age >18 years) per study and clear documentation of the type of implant used. The publication date had to fall between November 2014 and November 2024 to capture outcomes of contemporary surgical techniques and implants. Patients with underlying arthritic or pathological conditions, such as Paget disease, inflammatory arthritis, or tumor-related pathology, were excluded to maintain a trauma-only population. Studies were excluded if they were case reports, review articles, or focused on revision procedures, non-traumatic conditions, or hemiarthroplasty [Figure 1].

Screening Procedure
Two independent reviewers (KP, EU) screened all titles, abstracts, and full texts against the inclusion and exclusion criteria. Discrepancies were resolved by a third reviewer (AG). All reviewers were trained in systematic review methodology and were not blinded to study authorship or publication source. The methodological quality of included studies was assessed using the Newcastle-Ottawa Scale (NOS) for non-randomized studies and Cochrane RoB 2 tool for randomized clinical trials. This scale evaluates three domains: selection of participants, comparability of cohorts, and outcome assessment. Risk of bias assessments were performed independently by two reviewers, with disagreements resolved by consensus or by a third reviewer.
Data Extraction
Two reviewers independently extracted data using a standardized extraction form. The following variables were collected: study-level characteristics (including author, publication year, country, study design, sample size, and duration of follow-up), patient demographics (mean age and sex distribution), and surgical details (implant type and operative notes, when available). Functional outcome measures included the Mayo Elbow Performance Score (MEPS), Disabilities of the Arm, Shoulder, and Hand (DASH) score, and postoperative range of motion (ROM). Complication data were extracted across all studies and included infection, aseptic loosening, periprosthetic fracture, heterotopic ossification, mechanical failure, triceps insufficiency, and neuropathy. Further data were also extracted on the number and causes of reoperations or revisions in each study, which were defined as any surgical procedure that occurred after the original TEA involving the same elbow joint. If studies reported outcomes as medians or without standard deviations, appropriate statistical methods were applied to estimate mean values when feasible.
Statistical Analysis
A descriptive meta-analytic framework was used to summarize functional outcomes and complication rates. This study conducted a quantitative pooling of functional outcomes (DASH, MEPS, ROM) and complication rates using formal meta-analytic methods. A random-effects model was chosen a priori due to anticipated clinical and methodological heterogeneity among studies, including differences in study populations, surgical techniques, and follow-up durations. Pooled estimates were computed using a meta-proportion meta-analysis model to account for between-study variability. For continuous outcomes, pooled means with corresponding 95% confidence intervals were estimated using the `metamean()` function. For binary outcomes, pooled proportions were estimated using logit-transformed single-arm models via `metaprop()`. Study-level heterogeneity was quantified using the I² statistic. Sensitivity analyses were conducted by identifying and excluding studies whose confidence intervals fell outside the pooled estimate’s 95% limits, followed by recalculation of pooled effects. Results were recomputed after outlier exclusion to assess the robustness of conclusions. Publication bias was assessed using visual inspection of funnel plots, and Egger’s regression test was applied for outcomes with sufficient numbers of studies. Forest plots were also created to better visualize data. All meta-analyses were conducted in R (version 4.4.2) by a statistician affiliated with the Rothman Orthopaedic Institute.
RESULTS
After completion of the screening process, a total of 26 studies were included in the final analysis. Among these, 24 were cohort studies and two were randomized controlled trials. Collectively, the studies comprised 904 patients who underwent TEA for acute distal humerus fractures. Of these, implant type was reported for 830 patients (92%).
Risk of bias assessment using the NOS indicated that most cohort studies were at low overall risk of bias, with transparent reporting of patient selection and outcomes. Similarly, the two randomized controlled trials, assessed with the Cochrane RoB 2 tool, were at low overall risk of bias. The risk of bias assessment data is provided in Supplementary Material 2.
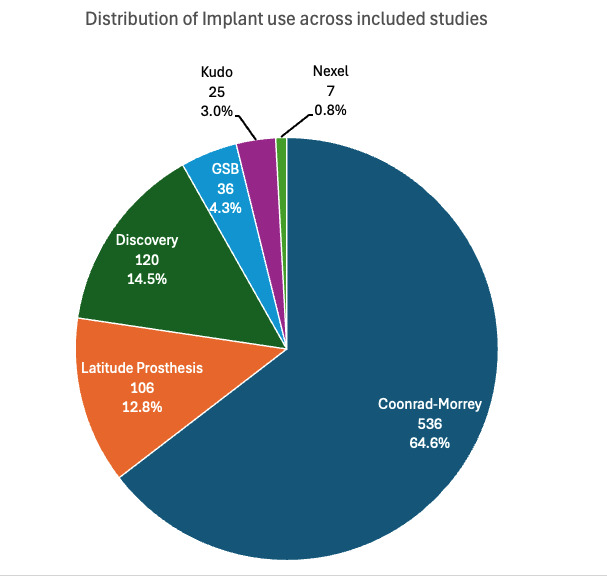
The mean age of the patient population was 74 years, and there was a marked predominance of female patients, who represented 88% of the total cohort. The most frequently utilized implant was the Coonrad-Morrey system (Zimmer-Biomet, Warsaw, IN), reported in 536 cases (65%). Other commonly used implants included the Discovery (Lima Corporate, Anduins, Italy) in 120 cases (15%), the Latitude (Wright Medical Group, Memphis, TN) in 106 cases (13%), the Gschwend-Scheier-Bähler (Sulzer Medical, Wintherthur, Switzerland) in 36 cases (4.3%), the Kudo (Stryker Howmedica Osteonics, Limerick, Ireland) in 25 cases (3.0%), and the Nexel (Zimmer-Biomet, Warsaw, IN) in 7 cases (0.8%) [Figure 2]. The mean follow-up duration across all included studies was 58 months, with a range from 3 to 156 months. Detailed study-level information is provided in Table 1.

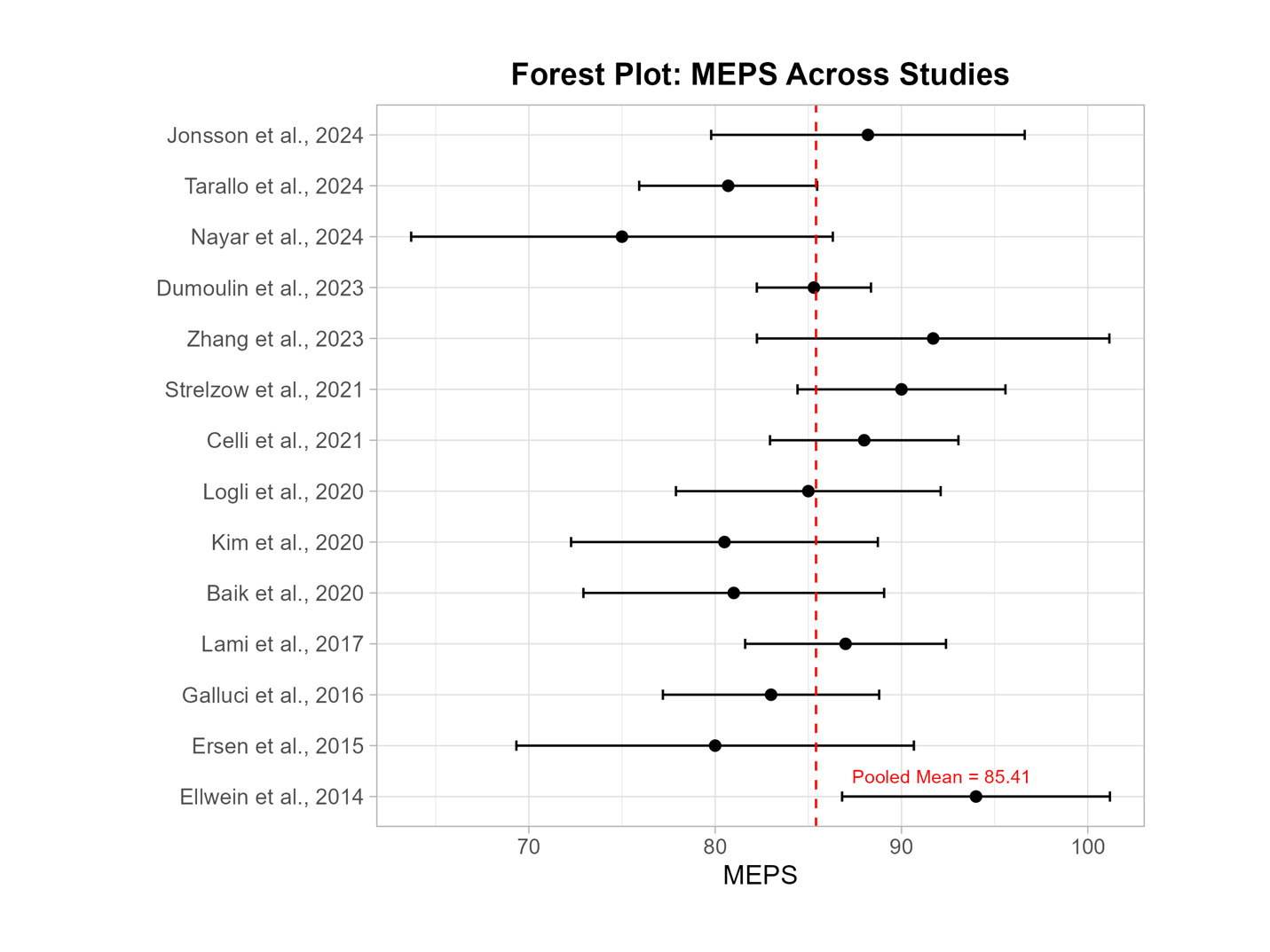
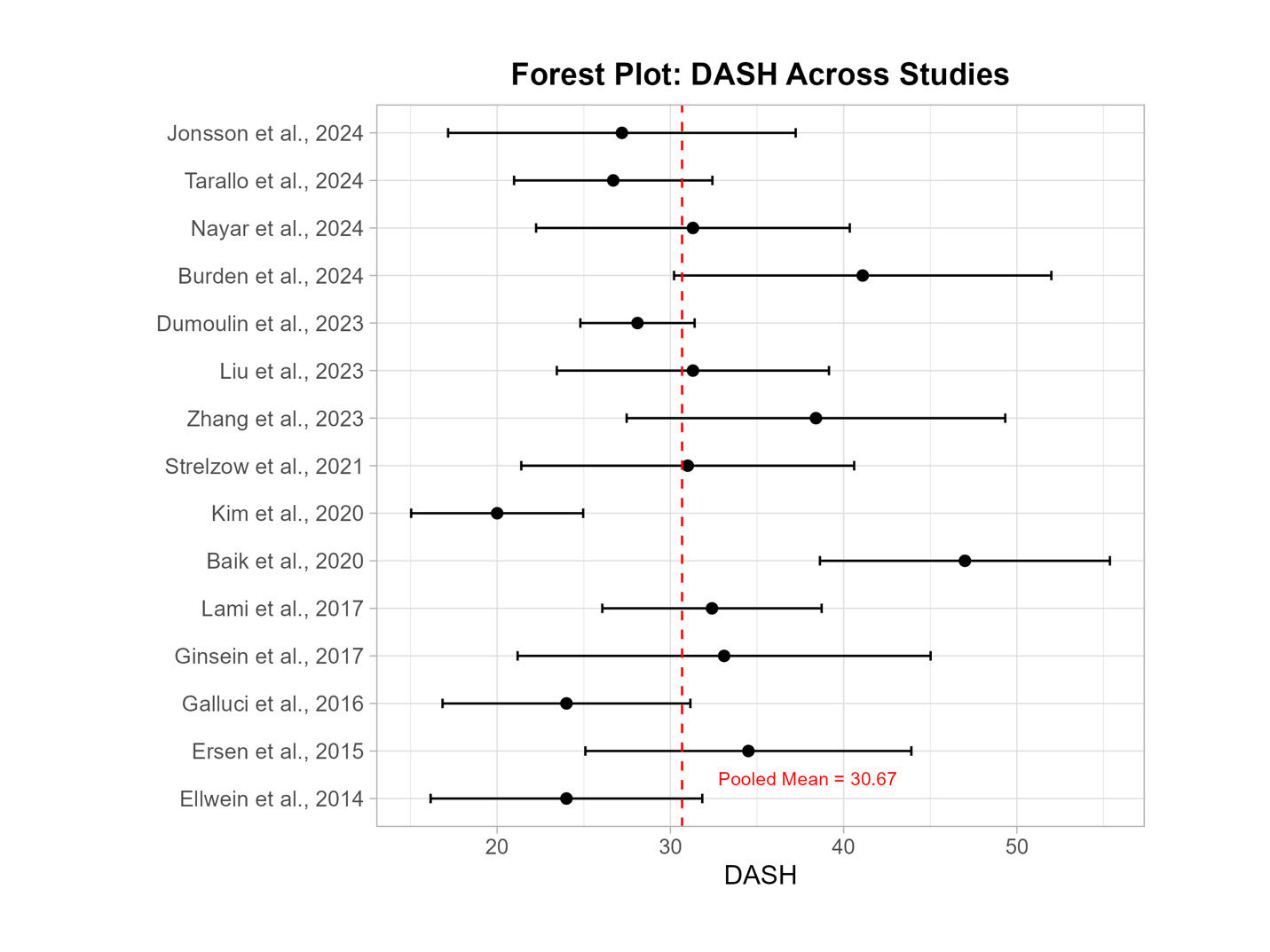
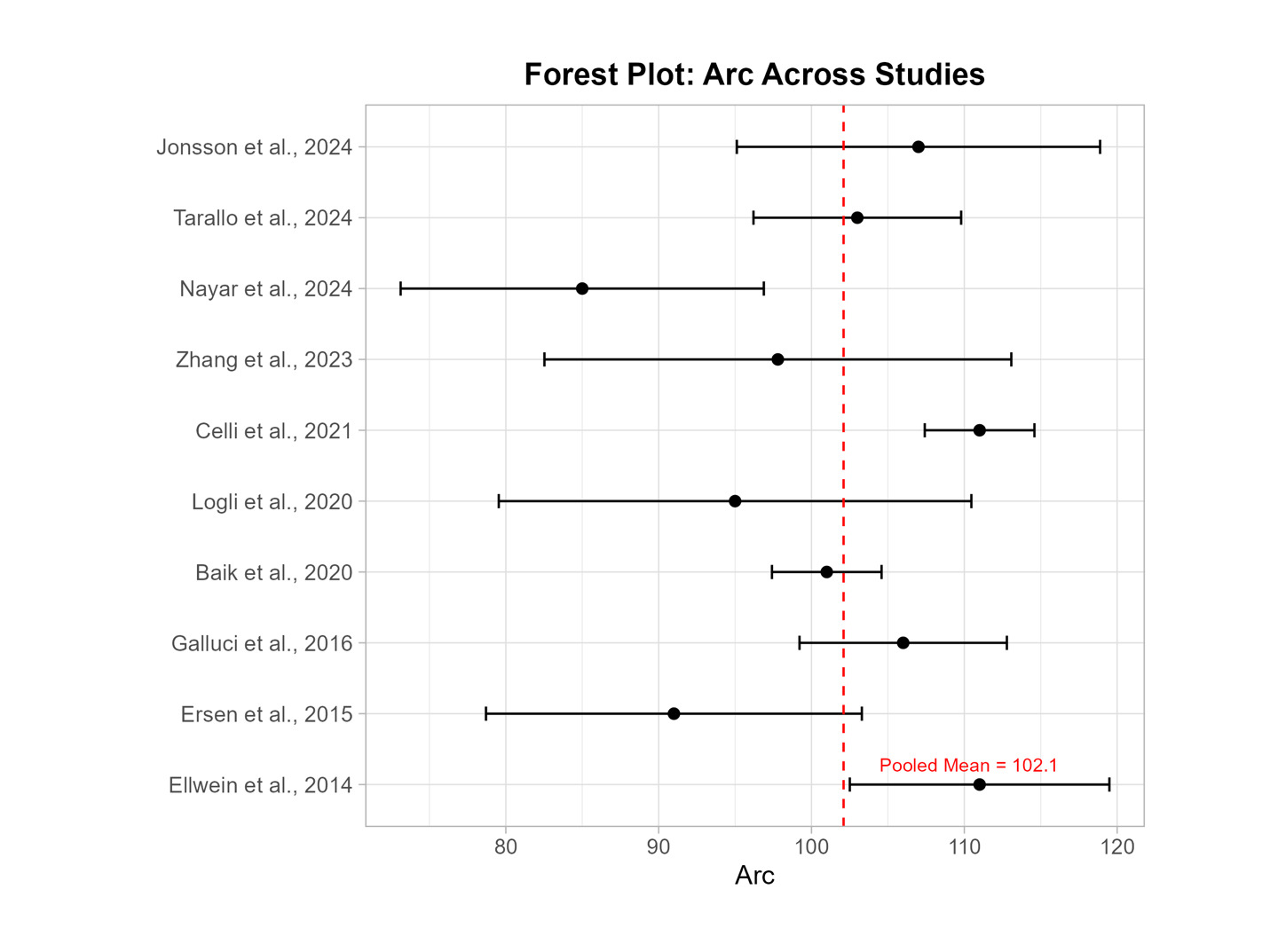
Functional outcome reporting varied across studies. Nineteen studies reported the MEPS, although only 14 of these included standard deviation data. The overall mean MEPS across studies was 86, while the pooled mean effect size was 85 [Figure 3]. Heterogeneity was assessed using the I² statistic; however, complete values for all outcomes were not uniformly available. After the exclusion of outlier studies identified through funnel plot analysis, the pooled mean MEPS slightly decreased to 85. DASH scores were reported in 16 studies, with 15 providing standard deviations. The overall mean DASH score was 32, and the pooled mean was 31 [Figure 4]. Following the removal of outlier studies, the pooled DASH score was reduced to 30.0. ROM outcomes were also commonly reported. The pooled mean values for postoperative elbow flexion and extension were 127° and 10.1°, respectively. After excluding outlier studies, the mean flexion was 125° and the mean extension was 13°. The flexion-extension arc had a pooled mean of 102° [Figure 5], which was adjusted to 101° after outlier exclusion. Study-level outcome data are summarized in Table 2. Outliers were identified based on visual inspection of funnel plots, and their exclusion resulted in minimal changes to pooled estimates, suggesting robustness of the findings. Publication bias was assessed for primary outcomes using funnel plots and Egger’s regression. No significant bias was detected.



A total of 210 complications were reported across all included studies, yielding a pooled complication rate of 23%. [Table 3] The most frequent complication was heterotopic ossification in 58 cases (28%). This was followed by infection in 35 cases (17%), both neuropathy and periprosthetic fractures in 28 cases each (13%), and aseptic loosening in 26 cases (12%). Additional reported complications included mechanical failure (17 cases, 8.1%), limited postoperative range of motion (15 cases, 7.1%), and triceps insufficiency (3 cases, 1.4%). Where reported, revision procedures included irrigation and debridement for infection, component revision for mechanical failure or aseptic loosening, and heterotopic ossification excision. These details were inconsistently reported across studies, which is noted as a limitation.
Revision or reoperation occurred in 74 cases, resulting in a rate of 8.2% out of all patients. [Table 4] Out of all complications, 35% led to reoperation or revision. The most common cause of revision/reoperation was infection, which accounted for 17 cases (23%). Other causes of reoperation or revision included mechanical failure (14, 19%), periprosthetic fracture (14, 19%), heterotopic ossification (11, 15%), aseptic loosening (11, 15%), neuropathy (4, 5.4%), limited postoperative range of motion (2, 2.7%) and triceps insufficiency (1, 1.4%).
DISCUSSION
In this systematic review and meta-analysis, the study focused on evaluating the current state of TEAs in the modern era, performed for acute distal humerus fractures, based on data from 904 patients across 26 studies published between 2014 and 2024. Analysis of this study’s results found that TEA remains a viable treatment option for complex distal humerus fractures in older adults, with favorable functional outcomes with a pooled mean MEPS of 85 and a flexion-extension arc exceeding 100°. However, this study’s overall reoperation/revision rate was 8.2%. Furthermore, the overall complication rate was over 23%, with heterotopic ossification, infection, and neuropathy being the most commonly reported adverse events. These results suggest that while TEA is functionally reliable in this patient population, it carries a considerable risk profile that warrants careful patient selection and surgical planning.
The demographic profile of patients undergoing TEA for acute distal humerus fractures in this review reflects established trends in the literature. Across the 904 patients included, the mean age was 74 years, consistent with prior reviews such as that by Kholinne et al.,6 who found that 72% of the patients in their studies were in the 70s. This stands to reason as bone mineral density decreases with age and is strongly correlated with fracture.32,33 This explains the higher likelihood of fracture after falls and acute injuries in elderly patients relative to their younger counterparts. This study also found that the majority of patients were female. Cawthon showed that osteoporosis, one of the biggest risk factors for distal humerus fractures, is much more prevalent in women- likely owing to the much lower bone mineral density in women relative to men.33 This results in a higher fracture risk.33 Another study reports that a 60-year-old woman has a 44% chance of fracture compared to a man of the same age who has a risk of 25%.34 These studies correlate with this one, explaining that the large majority of TEA patients are female.
This study also found that the vast majority of TEAs used the Coonrad-Morrey implant. Contemporary TEA implants are broadly categorized into linked and unlinked designs. Both systems comprise humeral and ulnar components but differ in terms of constraint and biomechanics. Linked implants incorporate a hinge mechanism that directly connects the components, offering inherent stability. In contrast, unlinked implants rely on soft tissue and bony integrity for stability, which may be insufficient in highly comminuted fractures. While unlinked designs may allow more physiological joint motion, they are generally reserved for less complex cases.35 The Coonrad-Morrey prosthesis has somewhat monopolized the TEA implant industry and has been the most popular option for surgeons internationally for years.36 Since its development and production in 1973, the prosthesis has been updated and modified a few times to improve its functional outcomes and reduce complication rates.37 Another systematic review conducted by Parker et al. also found their three most commonly used implants to be Coonrad-Morrey first, followed by the Latitude and Discovery prostheses, suggesting that these results are not uncommon.38
TEA seems to report high functional outcomes in both MEPS and DASH scores, 85 and 31, respectively, in this study. For MEPs, a rating of 75-89 can be described as good39 whilst for DASH, a score of 16-40 can be interpreted as an elbow that has a problem but is functionally working.40 These values indicate that although a TEA after a distal humerus fracture may not completely bring an elbow back to perfection and pre-injury state, the post-operative outcomes are favorable enough to result in a functional elbow for daily life. The ROM values, however, are subject to more debate. There does not seem to be a clear set of guidelines defining the normal range of motion of the elbow, likely due to the different range of motions required for various tasks. Some authors argue that up to 150° of full flexion is needed for “personal care, eating and drinking tasks”41 while another study argued that only the 75°-120° range of motion of the elbow was required for daily living.42 This discrepancy in guidelines does not allow this study to make a conclusive argument as to whether TEA works well in improving the functional outcome of the elbow after distal humerus fractures through all ranges of motion necessary for daily living.
The revision/ reoperation rate of TEAs in this study was 8.2%. This value is higher than reoperation rates for Total Knee Arthroplasties and Total Hip Arthroplasties, which a 2018 study found to be 1.2% and 2.05%, respectively.43 A possible explanation for this could be the volume with which each of these surgeries are performed. Prkic et al.44 compared the surgical volume of total elbow, knee, and hip arthroplasties in 2019 according to a Dutch database. The study found that in 2019, only 81 TEAs were performed compared to 25,859 total knee arthroplasties and 33,248 total hip arthroplasties.44 The significantly increased volume of knee and hip arthroplasties likely results in surgeons being more experienced in these surgeries, thus resulting in better outcomes and decreased reoperation rates. Unfortunately, whilst few studies in this review consistently reported and differentiated between the different types of reoperations. This study thus refrained from adding it in this current review, but it may be a point to make in future studies. Another point to note is that the results may have been affected by the smaller sample sizes and the number of TEA surgeries. This may have reduced the statistical power of the results, creating the difference seen in reoperation rates.
Other studies have noted high complication rates, including heterotopic ossification, infection, neuropathy, aseptic loosening, and periprosthetic fracture. Parker et al. found high rates of similar complications, although Parker reported their most common complication being aseptic loosening.38 This could be explained by their indications for TEA, which included arthritis, not just trauma. Degenerative diseases such as arthritis could lead to greater loosening, which could explain the disparity in results.
Whilst TEAs tend to have higher rates of complications compared to other joint replacement procedures, the rate of heterotopic ossification in this study seems to be similar or lower to that of different joints, such as hip replacement, for which one study reported a heterotopic ossification rate of around 25%.45 Toyoda et al.46 found a heterotopic ossification rate of 39% after primary total knee arthroplasties. Heterotopic ossification – formation of bone in soft tissue47- seems not to be related to the complexity of fractures, as other complications are. A possible explanation for this may be that greater weight-bearing joints, such as the knee and hip, are more likely to develop heterotopic ossification.
Over one in ten patients in this study suffered postoperative infections- a much higher rate than that of other arthroplasties, where studies suggest rates of 2.5% for hip arthroplasties48 and 4.4% for knee arthroplasties.49 Other significant complications included neuropathy, aseptic loosening, and periprosthetic fractures, all of which occurred in roughly one out of ten patients. Despite being lower than some of the other complications, these are still high rates that need to be reduced.
This current systematic review has several limitations. First, different studies reported different outcomes in different ways, making it difficult to compare the different studies and pool their results together directly. As part of this, the study acknowledges that functional outcomes may have been measured at different follow-up intervals. Whilst this may introduce bias in the results when pooled, outlier exclusion was completed to minimize this bias. Second, the lack of studies where only a single implant was used made it hard to compare the functional outcomes and complication rates between implants. Third, most studies selected were studies in which data were collected retrospectively, thus weakening the quality of data used in this systematic review. Also, findings in this study are limited to functional outcomes and reoperation rates, but not implant longevity or survival. Finally, like any systematic review, the quality of the study is limited by the quality and detail of the source studies.
CONCLUSION
This systematic review outlines the functional outcomes and complication rates of TEA. Despite its limitations, this study has highlighted that primary TEA for acute distal humerus fractures provides excellent functional scores and restores elbows to functional states after trauma. However, there is still a high rate of complications and reoperations, especially when compared to other arthroplasty surgeries.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
This study is a systematic review and meta-analysis of previously published data and does not involve any new studies with human participants or animals conducted by the authors. As such, ethical approval and informed consent were not required.
Declaration of informed consent
There is no identifiable patient information (names, initials, hospital identification numbers, images, or other personal data) included in this manuscript. Therefore, informed consent was not required.