INTRODUCTION
Proximal ulna fractures are a relatively common upper extremity injury. They can be broken down into olecranon process fractures, coronoid process fractures, and associated variant fractures of the proximal radioulnar joint.1 They make up approximately 20% of all proximal forearm fractures, with an estimated incidence rate of 12 per 100,000 people.2 The most common mode of injury is a fall from standing height, although younger patients are more likely to sustain injury with higher-energy mechanisms.1,2
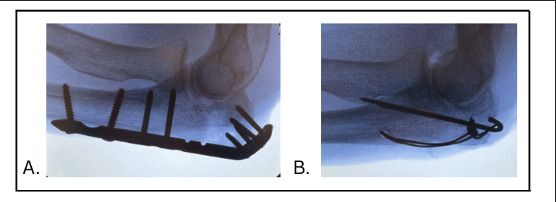
Olecranon fractures are often treated operatively, with treatment options commonly including but not limited to plate and screw fixation and tension-band wire fixation [Figure 1].3 Tension-band wiring has historically been indicated for minimally comminuted olecranon fractures without extension distally or involvement of the coronoid or shaft.4 It has had consistently good results, with 85% of patients reporting good or excellent results.5 However, tension-banding is known to cause hardware irritation, yielding meaningful removal rates.4,6 Alternatively, plate and screw fixation is a versatile fixation construct that can be used for simple as well as comminuted olecranon fractures and/or fractures with distal extension. Plate and screw fixation has also shown favorable outcomes.3,7
_plate_and_screws__and_(b)_tension-band_wiring.png)
Any hardware, particularly of the proximal ulna, can result in hardware irritation, warranting re-operation for hardware removal. There is ongoing controversy about hardware removal rates for various olecranon fracture fixation constructs. As such, this study’s primary goal is to determine the difference in hardware removal rates among plate and screw fixation vs other fixation strategies for operatively repaired olecranon process. The study hypothesis is that different olecranon fixation constructs will not have different hardware removal rates.
METHODS
The data used in this study were retrospectively queried on October 21, 2024, from the TriNetX United States Collaborative Network. This provides access to electronic medical records (diagnoses, procedures, medications, laboratory values, genomic information) from approximately 400 million patients across more than 220 healthcare organizations. This study is exempt from informed consent. The data reviewed is a secondary analysis of existing data, does not involve intervention or interaction with human subjects, and is de-identified per the de-identification standard defined in Section §164.514(a) of the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. The process by which the data is de-identified is attested to through a formal determination by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule. This formal determination by a qualified expert was refreshed in December 2020.8
Cohorts were divided based on International Classification of Diseases, 10th Revision (ICD-10) diagnosis codes. All patients diagnosed with displaced fractures of the olecranon process with intraarticular extension of the ulna and met criteria with ICD-10 codes S52.031A (right side) and S52.032A (left side), between January 1, 2017, and December 31, 2022, were included, resulting in 5082 patients. Patients with bilateral fractures or multiple procedures were treated as separate cases, as the TriNetX dataset does not allow for the identification of such patients across both sides.
Patient cohorts were then specified to have received operative treatment, using Current Procedural Terminology (CPT) code 24685 for open treatment of ulnar fracture, proximal end. They were then further categorized into “plate and screw” or “other fixation method” groups, representing tension-band fixation. The “plate and screw” group included patients with CPT code 24685 in addition to the ICD-10 code C1713, which is associated with an anchor/screw for opposing bone-to-bone or soft tissue-to-bone. The “other fixation method” group included patients with CPT code 24685 who did not have the associated ICD-10 code C1713. This group primarily represents tension-band wiring, but may consist of other fixation methods or miscoded procedures. The exact timeframe of January 1, 2017, to December 31, 2022, was queried, resulting in 1,195 patients in the plate and screw group and 1,399 in the other fixation method group.
Plate & screw, and other fixation method groups were further categorized based on subsequent evidence of hardware removal. This was done by using must-have and can-not-have functions of TriNetX using CPT codes 24160 and 20680.
Baseline demographic characteristics of all cohorts were then acquired, and statistical analysis was performed using the Analytics function of the TriNetX platform. This study did not adjust for fracture complexity, body mass index (BMI), comorbidities, or surgeon-specific factors, as the TriNetX dataset does not include detailed fracture classifications or patient-level data on these variables. Incidence was compared between cohorts using a 2-sided t-test to compare means, with a P value < 0.05 considered significant, while a Z-test was applied for comparing proportions. Odds ratios with 95% confidence intervals were calculated to determine associations between cohorts and incidence rates.
RESULTS
Demographic Trends
From 2017 to 2022, there were a total of 2,594 cases of an olecranon fracture that underwent operative treatment. The mean age of patients with olecranon fractures over the study period was 54 ± 25 years, with a significant decline in the mean age from 56 ± 25 years in 2017 to 54 ± 26 years in 2022 (P=0.026). Female patients represented a slight majority across all years, constituting approximately 53% of operative cases. There were no significant differences between genders in the proportion of operative cases from 2017 to 2022 (P=0.80).
Fixation Method and Hardware Removal Trends
From 2017 to 2022, there was a significant increase in the use of plate and screw fixation (36% to 48%; P<0.001), while the use of other fixation methods correspondingly decreased (64% to 54%; P<0.001). Across the whole study period, the overall rate of hardware removal after surgery was 19.9%. Plate and screw fixation had a hardware removal rate of 20.0%, while other fixation methods had a rate of 19.9%. The difference was not statistically significant (P=0.97), although we cannot conclude that the methods are equivalent based on this data. When broken down by race, gender, and age, there was a significant difference with age and gender, but not with race. When broken down by race, white patients saw similar levels of hardware removal as non-white patients (23% vs 21%), with a non-significant difference (P=0.28). When broken down by gender, 53% of removal cases occurred in males, while 47% of cases occurred in females (P=0.01). The rate of hardware removal was significantly higher in males compared to females (27% vs. 21%, P=0.01). Patients who had their hardware removed had a significantly younger mean age (49+/-24 vs 58+/-23, P<0.001). [Table 1]
DISCUSSION
This study analyzed hardware removal rates following surgical fixation of displaced fractures of the olecranon using data from 2017 to 2022. The study hypothesis was upheld; no difference in hardware removal rates was found between plate and screw fixation versus other fixation constructs. However, hardware removal rates were significantly higher in males compared to females.
Olecranon fixation hardware removal rates in this study were not significantly different for both plate and screw fixation (20.0%) versus other fixation methods (19.9%). Although we cannot conclude that the methods are equivalent, this finding is consistent with prior findings that hardware-related complications occur with all fixation techniques.4,6,9,10 However, our findings differ somewhat from prior literature that has often shown higher hardware removal rates in tension-band wiring compared to plate and screw fixation. For instance, Tarallo et al. showed hardware removal rates of 38% in tension-band wiring vs 17% in plate and screw fixation, while Duckworth et al. reported rates of 50% and 22%, respectively.6,10 Similarly, Steadman et al. also demonstrated a removal rate of 29% for tension-band wiring vs 20% for plates.11 Meta-analyses have confirmed this trend: Francis et al., pooling over 1100 patients from 15 studies, reported removal rates of 34% for tension-band wiring and 18% for locking plates, and Bethel et al. found similar results in a larger analysis (31% vs 14%).12,13
Our findings show less separation between fixation techniques, with comparable rates of plating removal to other studies, and lower rates of tension-band wiring. Several factors could explain why our findings show less separation between fixation techniques. Most notably, our study’s large, multicenter database sample may better reflect real-world variability in surgical technique, patient populations, and surgical thresholds. While increasing generalizability, this introduces potential confounders, as discussed below.
The lower tension-band removal rate may reflect evolving surgical practice patterns. In recent years, tension-band wiring has been reserved for less displaced or comminuted fracture patterns; this selective application of tension-band constructs may lead to lower rates of symptomatic hardware. More recent analyses tend to report tension-band removal rates hovering around 30%, as compared to higher rates in older studies.10–14
In contrast, hardware removal rates for plate fixation have remained relatively stable, possibly because plating is generally applied to a broader range of fracture complexities and patient populations. Overall, while prior literature consistently reported a higher rate of hardware removal with tension-band wiring compared to plating, our findings suggest that in contemporary practice, this difference could be narrowing.
While the data from this study showed no significant difference between fixation methods’ need for hardware removal, significant differences emerged when examining demographic factors. Young male patients had a significantly higher rate of hardware removal compared to females, potentially indicating differing tolerances for or thresholds to pursue hardware removal between genders. Contreras et al. studied risk factors for removal of symptomatic hardware and similarly found that those who underwent hardware removal tended to be younger.15 This age-related trend aligns with the possibility that younger, more active individuals may experience greater discomfort or irritation from retained hardware.
This study is subject to limitations inherent to large-scale database research. The reliance on coding may introduce bias, as diagnoses and procedures are contingent on proper documentation and patient engagement with the healthcare system. For example, we were unable to stratify by fracture complexity, BMI, comorbidities, or surgeon-specific factors, as the TriNetX dataset does not include detailed fracture classifications or patient-level data on these variables. This limitation may influence both the choice of fixation method and hardware removal rates. Also, because there was no ICD-10 code for tension-band wiring with sufficient data, we used all remaining olecranon fractures that were not coded as plate and screw as a proxy. While in most cases the fixation type would likely be tension-band wiring, it is possible that there were other methods used, or that plate and screw ICD coding was not done. The period studied (2017-2022) also encompasses the COVID-19 pandemic, which disrupted healthcare access and may have impacted surgical trends and follow-up care.
Despite these limitations, this study provides valuable insights into contemporary trends in olecranon fracture management. The shift toward plate and screw fixation emphasizes its growing role in surgical decision-making. At the same time, stable hardware removal rates across techniques suggest a need for continued focus on improving implant designs and surgical techniques to minimize complications. Future research should explore long-term functional outcomes and patient-reported satisfaction across fixation methods, as well as investigate disparities in access to surgical care.
CONCLUSION
This study highlights trends in the surgical management of displaced olecranon fractures, with increasing use of plate and screw fixation and comparable hardware removal rates between fixation methods. Within the cohort of patients undergoing operative treatment, there was a slight female majority, and the mean age was over 50 years. Hardware removal was significantly more common in younger and male patients. These findings reinforce the need for individualized treatment approaches based on fracture patterns and patient demographics, and less so for concern for fixation constructs relative to potential hardware removal.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
This study was exempt from the IRB review.
Declaration of informed consent
There is NO information in the submitted manuscript that can be used to identify patients.