Introduction
Total knee arthroplasty (TKA) is recognized as one of the most frequently performed and highly successful surgical interventions. It plays a crucial role in treating advanced knee osteoarthritis (OA), offering significant relief from persistent pain, limb realignment, and improved joint function.1 The effectiveness of TKA is contingent upon several critical factors, including thorough preoperative evaluations, precise surgical execution, and meticulous postoperative management. These elements collectively contribute to favorable patient outcomes and minimize complications.2
However, despite comprehensive preoperative planning, unanticipated findings not identified during routine assessments may arise intraoperatively. These incidental discoveries often complicate the procedure, requiring prompt, informed decision-making.3 Examples include soft tissue and bone tumors,1,4–10 which may be benign or malignant, and previously unrecognized anatomical abnormalities.11,12 Specific intraoperative findings, such as Ochronosis, tumors, or tuberculosis, may complicate the surgical process for knee arthroplasties.13,14
These incidental findings pose unique challenges, as their appropriate management often requires deviations from standard surgical protocols. Failure to address these anomalies before surgery could jeopardize the surgical outcome or result in subsequent complications.15,16 Therefore, awareness of the potential for such discoveries and developing strategies to manage them effectively during surgery is essential to ensuring optimal patient outcomes. By adopting a proactive approach to these unexpected findings, surgeons can modify their techniques to deliver the best possible results while maintaining the highest standards of patient care. No comprehensive review has systematically examined this topic in joint arthroplasty. This review aims to thoroughly evaluate reported incidental findings during TKA, detailing their occurrence, underlying pathophysiology, and appropriate management strategies.
Methods
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The study is registered in the PROSPERO database under the registration code CRD42024619341. The study focused on identifying patients who had unexpected findings during TKA that were not detected during routine preoperative assessments.
Search Strategy
A comprehensive literature search was conducted in the PubMed, Scopus, Embase, and Web of Science databases, covering the period from conception to December 2024. The search strategy utilized a combination of Medical Subject Headings (MeSH) terms and free-text keywords, specifically targeting (“knee arthroplasty” OR “knee replacement” OR “TKA”) AND (“Incidental Finding” OR “Incidental Discovery” OR “Unexpected”). Additionally, references from the selected studies and other relevant reviews were screened to identify further eligible studies.
Eligibility Criteria
Eligibility criteria were established to include methodologically robust and relevant studies. The review included only peer-reviewed original research articles, excluding book chapters, reviews, editorials, comments, and conference abstracts, to focus on empirically validated sources. No language or publication date restrictions were applied, ensuring a comprehensive temporal and linguistic scope. Only studies with accessible full texts were included; articles available solely as abstracts or with restricted access were excluded. These criteria enhanced the reliability, consistency, and comprehensiveness of the review findings.
Study Selection
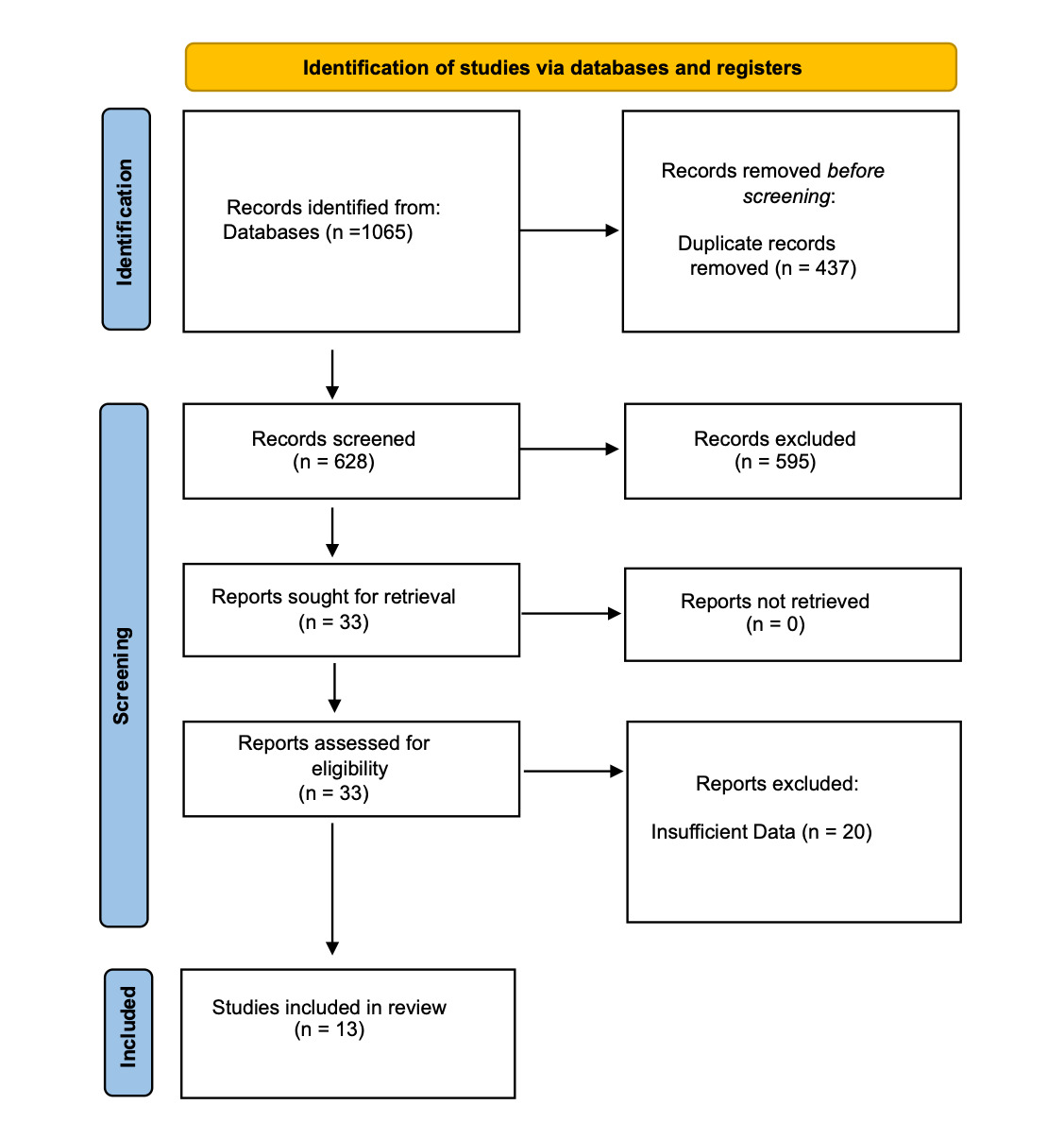
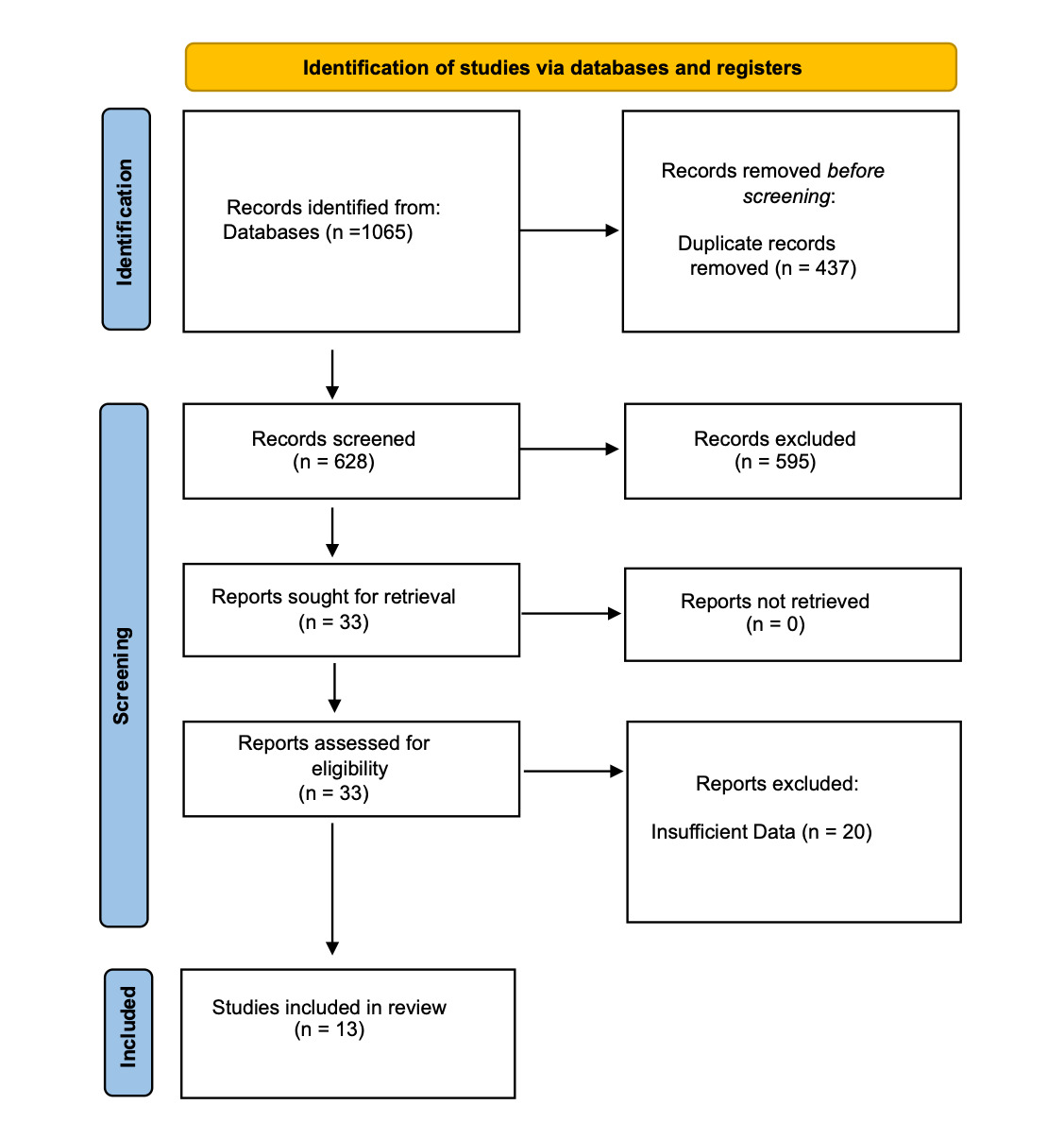
Two reviewers (MS and DR) screened titles and abstracts independently to identify potentially relevant studies. Full-text articles were retrieved for those meeting the inclusion criteria or where eligibility was unclear. Final inclusion was determined following an independent assessment by the reviewers, with disagreements resolved through discussion or consultation with a third reviewer (AP). A PRISMA flow diagram illustrates the study selection process [Figure 1].
Quality Assessment
The quality of the included studies was evaluated using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist [Tables 1 and 2], tailored to the study design. Each study was assessed across key domains, including Selection bias, Reliability of measurements, Control of confounding factors, Completeness of outcome data, and Clarity of reporting findings. Studies were categorized as high, moderate, or low quality based on these criteria. To enhance inter-rater reliability and reduce subjectivity, two independent reviewers conducted the quality assessments, with any disagreements resolved through discussion or consultation with a third reviewer. This standardized approach ensured transparency and rigor in the quality evaluation process.
Data Extraction and Synthesis
A systematic data extraction process was employed using a standardized form to capture essential information, including study design, sample size, participant demographics, intervention characteristics, outcome measures, and primary findings. Two reviewers independently performed data extraction to minimize bias, resolving discrepancies through discussion or consultation with a third party (AM). Given the heterogeneity in study designs and outcomes, a narrative synthesis approach was adopted. Studies were categorized thematically, and findings were synthesized to identify key patterns, trends, and variations. This method facilitated a structured and comprehensive analysis of the available evidence.
Results
The systematic review identified a total of 1,065 articles, with contributions from PubMed (504 articles), Scopus (431 articles), Embase (154 articles), and Web of Science (176 articles). Duplicate records were removed, resulting in the exclusion of 437 articles. Subsequently, the titles and abstracts of the remaining 628 articles were screened, applying predefined exclusion criteria to eliminate studies with inappropriate methodologies or participant populations. This screening process excluded 595 articles, leaving 33 studies for full-text evaluation. Following a thorough assessment, 13 studies were deemed eligible for inclusion, comprising a total of 26 patients.
Most patients were female (18 vs. 8), aged 48 to 77. Apart from those with alkaptonuria and tuberculosis, no patients reported extra-articular knee symptoms before undergoing TKA. Except for a case of Ochronosis, all surgeries were performed in a single session without postponement. The primary indication for TKA was degenerative conditions, primarily osteoarthritis, though other causes, such as trauma and congenital joint abnormalities, were also noted. Additionally, incidental findings, including tumors, synovitis, and other pathological conditions, were frequently observed, highlighting the need for thorough preoperative evaluations to identify coexisting abnormalities. Table 3 summarizes the included studies and patient characteristics, detailing demographic data, primary indications for TKA, and incidental findings identified during preoperative evaluations.
Discussion
TKA is a commonly performed and successful surgery. However, incidental findings can complicate the procedure, even in the absence of symptoms or signs detected during routine preoperative assessments. Ensuring excellent preoperative assessment, accurate perioperative procedures, and thorough postoperative follow-up is crucial to effectively addressing these complications.
Some findings in TKA, such as tenosynovial giant cell tumor (TGCT), have case series available. On the other hand, findings such as lipoma arborescens, metastatic mammary carcinoma, black cartilage, synovial sarcoma, non-Hodgkin lymphoma, and tuberculosis of the Joint only have case reports available.
Tenosynovial Giant Cell Tumor (TGCT)
Diagnosing TGCT during TKA can be challenging because it can mimic other joint diseases, such as osteoarthritis.22 Accurate identification often occurs only during surgical intervention.23 TGCT can be categorized into two types: localized type (L-TGCT), characterized by focal tuberculous hyperplasia in the synovium, and diffuse type (D-TGCT), which involves thickening of the entire synovium with diffuse joint effusion.24,25 Early-stage diagnosis is difficult due to atypical presentation and the absence of specific laboratory tests. Therefore, a combination of imaging techniques, such as X-ray, magnetic resonance imaging (MRI), and computed tomography (CT) scans, with MRI as the primary modality, is often necessary for visualization and assessment.24,26–28 Treatment typically involves tumor resection, possibly with simultaneous biopsy for frozen section pathological analysis, or later, along with adjuvant therapies such as radiation or chemotherapy to reduce recurrence risk.28,29 In advanced stages with destructive lesions, arthrodesis or TKA may be preferred.30 Further research is needed to enhance the understanding of TGCT and improve treatment strategies.30
In a study, Lei et al.22 reported 10 female patients with osteoarthritis who underwent TKA. Red and brown synovial lesions were discovered during surgery and later confirmed as TGCT by histopathological analysis. Common symptoms among the patients included joint pain, limited range of motion, and difficulty in activities such as stair climbing and squatting. Their white blood cell and neutrophil granulocyte counts were within normal ranges. Elevated erythrocyte sedimentation rate (ESR) was observed in 7 patients, and three had elevated C-reactive protein (CRP). For the treatment of L-TGCT, partial synovectomy was performed, while complete synovectomy was conducted for D-TGCT. At the last follow-up, significant improvements were observed in knee KSS and function scores compared to the preoperative values. In this study, TGCT was diagnosed intraoperatively during TKA based on suspicious synovial appearance and confirmed postoperatively by pathology. Additional synovectomy was performed at the time of TKA; no separate procedures were required.
TGCT and OA can present similarly, but MRI can help distinguish TGCT by revealing characteristic soft tissue features. Elevated ESR/CRP may be seen in TGCT, but they are nonspecific. Advanced imaging is not routinely needed for all patients with elevated markers—clinical judgment remains key.
Lipoma Arborescens
Lipoma arborescence is a synovial tumor characterized by the growth of adipose tissue within the synovium, resulting in inflammation and hyperplasia. It can manifest as idiopathic or secondary, with the latter associated with pathologies such as osteoarthritis, diabetes mellitus, senility, and rheumatoid arthritis.31,32 A clinical case by Alshehri et al.33 described a 64-year-old male with persistent bilateral knee pain for six years. Arthrotomy revealed a thickened synovium with accumulated synovial fluid, confirming the diagnosis of bilateral lipoma arborescens. Surgical excision of the lipoma, synovectomy, and TKA yielded successful outcomes without complications. This approach has demonstrated efficacy in providing long-term symptom relief.34,35 Although lipoma arborescens can present with clinical features resembling primary osteoarthritis, such as synovial thickening and joint effusion, the defining characteristic is fatty infiltration within the synovium, often with a “tree-like” morphology. Routine histopathologic examination of synovial tissue during TKA may not be warranted in all cases. However, when intraoperative findings raise suspicion, such as abnormal, yellowish, or lobulated synovial tissue, sending the specimen for pathology can help identify rare conditions like lipoma arborescens and guide long-term management.
Metastatic Mammary Carcinoma
The fortuitous discovery of metastasis of breast adenocarcinoma to the knee during TKA is a rare and significant occurrence.1 Breast cancer commonly spreads to the bones, with the vertebrae, femur, humerus, ribs, skull, sternum, and pelvis being frequent sites of metastasis.36,37 It is worth noting that bone metastases often present with pain as the initial symptom, and radiographic evidence may not be evident in the early stages of the disease.38
In this particular case,1 a 70-year-old woman presented with persistent pain localized to her right knee. Preoperative knee radiographs showed degenerative changes but no signs of metastatic pathology. Physical examination revealed a valgus deformity in the right lower extremity, with no other notable findings. During TKA and subsequent histopathological examination, neither the operating surgeon nor the pathologist identified any abnormalities during the gross inspection of surgical specimens. The presence of tumor cells was detected solely by histological scrutiny. Subsequent evaluation confirmed the presence of a tumor in the right breast, indicating metastatic breast cancer. The patient underwent chemotherapy and adjuvant radiation therapy targeting the spine and hip. Unfortunately, the patient passed away approximately eighteen months after hospitalization. This case underscores the importance of comprehensive preoperative evaluation, especially in elderly patients or those with vague symptoms. While metastatic disease may not be apparent on routine imaging, advanced modalities (e.g., MRI, CT, positron emission tomography (PET)) should be considered in high-risk individuals such as a personal history of malignancy (e.g., breast, lung, prostate, kidney, thyroid), unexplained weight loss, night sweats, fatigue, Abnormal imaging findings, or lab values not typical of osteoarthritis. Additionally, intraoperative suspicion and biopsy of unusual bone quality or lesions may aid in the early detection of occult malignancies.
Non-Hodgkin Lymphoma
Non-Hodgkin lymphoma (NHL) can involve bone in 5-25% of cases, leading to joint pain.39,40 In the initial study by Watson et al., a 60-year-old male presented with chronic right knee pain. During TKA, the surgeon observed a dark gray appearance of the patient’s femur but a normal tibia. Microscopic examination showed atypical marrow with normal bony trabeculae. Histological analysis revealed low-grade malignant B-cell lymphoma involvement in the marrow, even though the patient had no lymphoma symptoms.
In a study by Visser et al., a 69-year-old female patient with rheumatoid arthritis underwent left TKA due to advanced arthritis.40 The patient presented with a correctable valgus deformity of the left leg, mild knee effusion, and tenderness upon palpation of the lateral joint space. During the surgical procedure, pigmented vitreous synovial tissue was found in the subcutaneous layer and subsequently excised for further analysis, leading to a diagnosis of NHL. The TKA was completed without complications, and the patient was discharged five days postoperatively. Although long-term outcomes were not detailed, the reports emphasize the importance of ongoing hematologic follow-up after the discovery of incidental lymphoma. Preoperative identification remains challenging in asymptomatic patients but can be aided by a detailed clinical history, assessment for constitutional symptoms, targeted imaging (e.g., MRI or PET in cases of unexplained joint pain), laboratory evaluation, and consideration of synovial biopsy when atypical intra-articular findings are present.
Ochronosis (Black Cartilage)
Alkaptonuria, first described in 1908, is one of the earliest recognized inborn errors of metabolism. It results from mutations in the homogentisate 1,2-dioxygenase (HGD) gene, leading to a deficiency of the HGD enzyme, which breaks down homogentisic acid. The accumulation of HGA in cartilaginous tissues causes a distinctive bluish-black discoloration known as Ochronosis. Although Ochronosis is generally asymptomatic, it often leads to ochronotic arthropathy due to pigment deposition in joints.41
Ochronosis is a rare metabolic disorder characterized by the accumulation of homogentisic acid (HGA) in connective tissues,42 resulting in a distinct bluish-black pigmentation of the skin, cartilage, and sclera.19,43,44 This condition can present as joint stiffness, arthritis, and degenerative changes in the spine and large joints.42 During a TKA, Kumps et al.45 made an unexpected discovery. Upon exposing the joint capsule, the surgeon noticed a brown-black discoloration of the cartilage, prompting a postponement of the surgery for further investigation. Subsequent tests confirmed elevated levels of homogentisic acid in the urine, as well as bilateral Ochronosis of the ear cartilage, sclera, and teeth, accompanied by a hyperpigmented postoperative scar. The TKA was performed later without any complications. It is important to highlight that treatment options for Ochronosis are limited, primarily focusing on symptom management rather than providing a definitive cure.46
In a case reported by Chang et al.,20 a 77-year-old man with no significant medical history presented with chronic mechanical knee pain. A radiographic examination revealed degenerative arthritis, and he underwent total knee arthroplasty. During the surgery, bluish-black pigmentation of the bone and cartilage was observed, consistent with Ochronosis. The surgery and recovery were uneventful, and the patient was later diagnosed with alkaptonuria, a previously unrecognized rare metabolic disorder. Similarly, in a case described by Visser et al.,12 a 52-year-old man with knee osteoarthritis underwent knee replacement surgery. During the procedure, black discoloration and early cartilage degeneration were noted, characteristic of alkaptonuria due to HGA accumulation. These cases underscore the clinical challenges in diagnosing and managing this rare metabolic condition, particularly when it presents during joint replacement surgery.
A detailed clinical history is essential for preoperative identification of Ochronosis, particularly regarding the presence of dark urine or pigmentation. Physical examination should assess for bluish-black discoloration in the ears, sclera, or teeth. Urine homogentisic acid testing can confirm the diagnosis, and advanced imaging or arthroscopy may reveal early joint changes that suggest ochronotic arthropathy.
Black Bone
Intraoperative discovery of discolored bone during TKA can perplex surgeons and raise concerns. Discoloration may stem from various causes, including Ochronosis, metabolic bone diseases, metal deposits, sequestrum, metastatic disease, or drug-related pigmentation, such as that induced by minocycline. In a case by Reed et al.,19 a 55-year-old woman undergoing TKA revealed pigmented bone attributed to minocycline use, highlighting a rare but significant finding for orthopedic surgeons. The implications of minocycline-induced pigmentation on bone metabolism and structural integrity remain poorly understood. However, recognizing this phenomenon is crucial for informed intraoperative decision-making, particularly regarding component selection and fixation in joint arthroplasty. Awareness of such side effects can help surgeons manage unexpected findings effectively.
Synovial Sarcoma
Synovial sarcoma, a type of soft tissue sarcoma, predominantly affects individuals aged 15 to 35, accounting for 5 to 10% of all sarcomas.47 This malignancy manifests near the large joints of the lower limb as a slow-growing mass.48,49 Despite characteristic imaging features, such as a calcified soft-tissue mass and a heterogeneous “triple signal” on T2 MRI sequences, early diagnosis and effective disease management remain challenging.50,51 In a case reported by Savvidou et al.,50 a 68-year-old female patient with chronic right knee pain underwent TKA, where surgeons unexpectedly observed thickening of the synovial membrane and an associated “fat mass.” Further examination revealed a biphasic malignancy of spindled mesenchymal cells and glandular epithelial elements. Standard treatment for synovial sarcoma involves wide resection and adjuvant radiotherapy, with chemotherapy potentially improving survival rates. The reported 5-year survival rates range from 30 to 74%.48,52 In this case, an en bloc tumor resection and revision TKA with a megaprosthesis were performed 28 days after the primary TKA. Regional neurovascular structures were preserved, and the resulting bone defect was reconstructed using a modular knee megaprosthesis.50
Osteoarticular Tuberculosis
Osteoarticular tuberculosis primarily targets large joints, with the knee joint being the least affected. This condition is more prevalent in developing countries.53 Misdiagnosis often occurs in patients with primary knee osteoarthritis or other conditions, which complicates the identification of underlying tuberculosis.21,54 Wang et al.55 reported four cases of knee joint tuberculosis initially misdiagnosed as rheumatoid arthritis (RA), osteoarthritis, and Charcot’s arthropathy. Patients presented with localized knee joint swelling and pain without systemic symptoms. Preoperative assessments showed elevated levels of CRP and ESR and positive rheumatoid factor (RF) in one case. Radiographic findings revealed various abnormalities, including osteoporosis, bone destruction, subluxation, and soft tissue swelling. Postoperative diagnoses confirmed tuberculosis through pathological examinations, polymerase chain reaction detection, acid-fast staining, and next-generation sequencing.56
In a study by Yamazaki et al.,21 two cases of knee joint tuberculosis were identified following TKA. Preoperatively, one case was misdiagnosed as RA and the other as osteoarthritis. In the first case, the diagnosis was established postoperatively by culture of pus from a sinus tract. In contrast, in the second case, tuberculosis was confirmed via pathological analysis of synovial tissue obtained during surgery. Retrospective analysis indicated that a thorough review of family and medical history, combined with careful radiographic examination, could have facilitated an accurate preoperative diagnosis in both cases. Treatment outcomes were favorable, with resolution of inflammation achieved through anti-tuberculous therapy and surgical debridement in the first case and through anti-tuberculous therapy alone in the second. These findings suggest that knee joint tuberculosis can be effectively managed with anti-tuberculous medications and debridement, even in patients with prosthetic implants.
Gouty Arthritis
Subchondral cyst formation is frequently observed in patients with OA and RA.57 While RA is known to cause large synovial cysts, often called geodes, extensive subchondral cysts associated with pseudogout-induced OA are rare.58 Mittl et al.18 reported a case involving a 65-year-old male with a history of gout and bilateral knee pain who underwent left TKA. Despite preoperative radiographic imaging showing no evidence of gouty tophi, intraoperative findings revealed a distinctive chalky white paste consistent with monosodium urate (MSU) crystal deposition on the articular surfaces of the knee, confirming gouty arthritis. This case underscores the under-recognition of gouty arthropathy in arthroplasty patients. Preoperative identification can be improved through thorough history-taking, physical examination for tophi, serum uric acid testing, synovial fluid analysis, and advanced imaging such as ultrasound or dual-energy CT.
Intraoperative Management Strategies
A structured, evidence-informed approach can guide intraoperative decision-making when unexpected findings are encountered during TKA.3,15 Incidental discoveries may be classified into three general management pathways, depending on their nature and potential impact on patient outcomes.3,16 In cases where findings are clearly benign and do not compromise implant safety, such as ochronosis, minocycline-induced pigmentation, or gouty tophi, the procedure may “proceed as planned”, with careful documentation and confirmatory histopathological analysis.19,20 If there is suspicion of malignancy, including entities such as synovial sarcoma, lymphoma, or metastatic carcinoma, intraoperative frozen section or biopsy should be prioritized, and definitive prosthesis implantation “deferred until full oncologic workup” and multidisciplinary planning are completed.1,5,7,17 In situations where features strongly suggestive of active infection are present, such as purulence or caseating granulomas seen in osteoarticular tuberculosis, the safest course is to abort the procedure, obtain appropriate cultures, and initiate targeted antimicrobial therapy, with “delayed reimplantation” considered as part of a two-stage protocol.14,21 This framework emphasizes intraoperative vigilance and patient safety, ensuring that prosthesis implantation is reserved for appropriate clinical conditions.2,3
Preoperative Indicators of Atypical Pathology
While most incidental findings during TKA are not detected through standard preoperative evaluation, several subtle clinical, laboratory, and radiographic indicators may justify further investigation.2,8,59 A comprehensive patient history is essential, as a prior diagnosis of malignancy, particularly involving the breast, prostate, lung, kidney, or thyroid, along with a history of gout, metabolic disorders, or known tuberculosis exposure, should prompt heightened diagnostic vigilance.1,5,11,14,18 Clinically, features such as pain disproportionate to radiographic findings, recurrent or unexplained effusions, and constitutional symptoms, including fever, night sweats, or unexplained weight loss, may suggest underlying pathology beyond primary osteoarthritis.4,7,17,21 Laboratory abnormalities, such as elevated ESR or CRP in the absence of overt infection, may indicate conditions like tenosynovial giant cell tumor (TGCT) or osteoarticular tuberculosis, warranting further assessment with synovial fluid analysis or advanced imaging.8,60 Recognizing these preoperative “red flags” may improve diagnostic accuracy, facilitate earlier identification of atypical conditions, and enhance surgical planning and intraoperative preparedness.2,8,59 [Table 4]
Limitations
This review is limited by the available literature, which primarily consists of case reports with minimal follow-up, making it challenging to assess complications and long-term outcomes. Despite millions of TKAs performed during the study period, the small number of reported incidental findings suggests likely underreporting, as many incidental findings may go undocumented if they do not alter surgical management. Variability in reporting standards further limits the ability to draw broad conclusions. Plausible reasons for underreporting include the clinical insignificance of incidental findings that do not affect management, medicolegal concerns about documentation, and publication bias or a lack of suitable forums for reporting intraoperative discoveries. These factors reflect systemic barriers to comprehensive data collection and underscore the need for broader and more standardized reporting in future research to clarify the true incidence and clinical impact of these findings.
Conclusion
Incidental findings during TKA are occasionally encountered despite unremarkable preoperative assessments. As demonstrated by various reported cases, including metastatic disease, non-Hodgkin lymphoma, Ochronosis, and gout, many of these conditions are difficult to identify preoperatively due to nonspecific clinical presentations or the absence of systemic symptoms. While enhanced screening methods such as advanced imaging, synovial fluid analysis, and detailed history-taking may improve detection in selected cases, most of these findings remain unsuspected until intraoperative discovery. These observations underscore the importance of maintaining a high index of suspicion, conducting careful intraoperative assessments, and performing appropriate postoperative histopathological evaluations to inform optimal surgical decision-making and patient management.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
No ethical approvals required for this work.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.