INTRODUCTION
Hip fractures are relatively common injuries with an estimated 260,000 to 300,000 cases in the United States (US) annually.1 These injuries often present after low-energy falls in the elderly, and to a lesser extent, high-energy trauma in younger patients.2–4 Hip fractures contribute to considerable morbidity and mortality in the population, generally requiring hospitalization, surgical management, and a potentially protracted recovery. Estimates of permanent disability with loss of ambulatory function or level range from 30-50%, and mortality one year following a hip fracture is reported to range from 2-34%.5,6 In addition to disrupting quality of life, these injuries impose substantial costs on both patients and health care system. A hip fracture injury is estimated to cost between $48,000 and $60,000 within the first year after surgery.7–9 This equates to tens of millions of dollars spent on treating these injuries each year, placing a meaningful strain on the US health care system.
Treatment for femoral neck fractures (FNFx) includes open reduction-internal fixation (ORIF) via pinning, hemiarthroplasty (HHA), total hip arthroplasty (THA), and occasionally, non-operative palliative care.2,10 Treatment selection is based on fracture and patient characteristics. Traditionally, ORIF fixation utilizing partially threaded cannulated screws, often referred to as “hip pinning,” has been indicated for non- or minimally displaced FNFx, where the vessels perfusing the femoral head are more likely to be preserved. In contrast, arthroplasty is generally used in cases with a displaced FNFx, where perfusion of the head is likely compromised, reducing its ability to heal with fixation. Specifically, HHA has been most commonly used for the management of displaced FNFx, eliminating the potentially devascularized femoral head and restoring hip mechanics without altering the acetabulum. Recently, there has been an increasing trend toward using THA over HHA for displaced FNFx, with theoretical advantages of improved longevity and a lower reoperation rate.11 However, the use of THA versus HHA may entail longer surgery, higher implant costs, and greater risk of instability and prosthetic revision.12,13
Given the high prevalence of FNFx and its associated high costs and morbidity, there is value in further characterizing trends in management. The study hypothesis is that THA operations are increasing over time relative to HHA for displaced FNFx.
METHODS
A retrospective study was performed utilizing the TriNetX US Collaborative Network. The TriNetX database does not contain patient-identifiable information and is therefore exempt from Institutional Review Board review and approval. TriNetX is a global research network encompassing data from over 170 healthcare organizations and more than 400 million patients. It contains de-identified, aggregated patient information on procedures, diagnoses, medications, vitals, genomics, and demographics. Healthcare Organizations (HCOs) involved in the TriNetX network contribute healthcare data in de-identified, pseudo-anonymized, or limited-data-set formats, in accordance with local privacy regulations. These HCOs authorize the usage of this data for research purposes on the TriNetX platform. In return for providing data, HCOs incur no financial expenses and gain access to data query tools, analytics, visualization capabilities, and the necessary hardware for software execution. The de-identification process conforms to Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule standards, as verified by a qualified expert, meeting the requirements of Section §164.514(b)(1), ensuring HIPAA compliance.
Subjects were identified as having a femoral neck fracture with International Classification of Diseases, Tenth Revision (ICD-10) code S72.0 in addition to one of the operative Current Procedural Terminology (CPT) codes within one month of injury [Table 1]. Patients included were aged 65 to 90 years and from 2017 to 2022. Cohorts were further defined by having received pinning (ORIF), hemiarthroplasty (HHA), or total hip arthroplasty (THA). An additional cohort was created by combining HHA and THA for an arthroplasty-only group. Cohorts were compared over time and stratified by age and gender. Additionally, arthroplasty was compared to pinning, and THA was compared to HHA. Native Hawaiian/Pacific Islander and American Indian/Alaska Native racial groups were excluded due to low sample sizes, as well as unknown sex, ethnicity, and race.
RESULTS
A total of 30,906 patients were identified as having one of the operations of interest after a femoral neck fracture during the study period [Table 2]. Of patients with their gender reported in the operative group, 67% were females compared to 33% males. Yearly rates for males and females did not change over time. Overall, females outnumbered males by almost double.
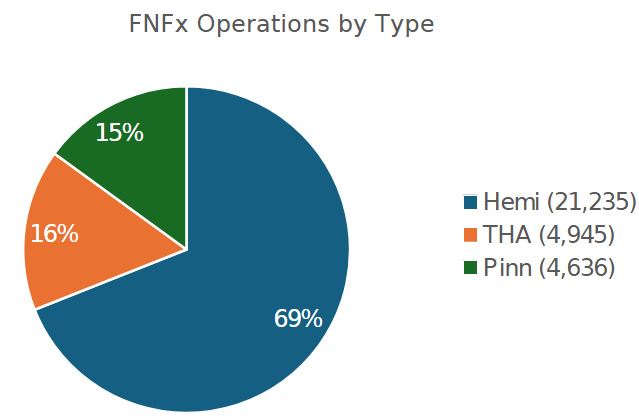
Arthroplasty was used far more frequently than ORIF in the surgical management of all FNFx (P<0.001) over the study period, with 85% versus 15%, respectively [Figure 1]. Moreover, annual utilization trends changed over time. Over the study period, yearly incidence demonstrated small but significantly increased utilization of THA (P<0.001) [Table 3] and significantly decreased utilization of arthroplasty in general for all FNFx (P<0.001) [Table 4]. These trends were found to be consistent relative to gender as well.

DISCUSSION
This study aimed to assess changes in the utilization of FNFx operations. The study hypothesis was upheld, with statistically significant increased utilization of THA for displaced FNFx relative to HHA. Moreover, while THA incidence increased, the use of both HHA and ORIF decreased over the study period.
From 1990 to 2001, Jain et al. examined surgical utilization trends for FNFx in the US and found that HHA was the most common operation performed and increased in prevalence during this period, while THA and ORIF were less commonly performed.14 Since then, however, THA has become increasingly utilized for FNFx.15–17 This increase in THA usage is supported by several studies that find improved quality of life with similar infection and reoperation risks when comparing THA to HHA.15,16,18,19 This study’s findings underscore changes in the utilization of these operations. Current analysis demonstrates a higher utilization rate of THA than those examining earlier time periods. It is speculated that this may be due to possible advances in surgical technology and changes in surgeon preferences.
It should be noted that while the increase in THA utilization is statistically significant, the absolute change is modest. This likely reflects incremental rather than transformative change in national practice patterns. However, even small shifts on a large scale may signify growing comfort with THA for FNFx. And as evidence evolves, it may be particularly favored for use in select patient populations.
In addition, HHA can be indicated for non-displaced or minimally displaced FNFx injuries. This study confirms increased utilization of HHA and THA over ORIF over the study period. This is consistent with previous studies demonstrating primary HHA has better outcomes than secondary HHA following prior ORIF.20,21 As many as 10% of pinning operations have been shown to need conversion to HHA within 5 years in a Swedish registry for patients over 60 years of age with a non-displaced FNFx.22 As the body of evidence continues to favor arthroplasty, an increased trend for arthroplasty, including THA, can be anticipated for displaced FNFx.
Despite several novel findings in this study, it is not without limitations. Foremost, the present study aimed to identify trends in the utilization of surgical procedures for FNFx. However, did not attempt to elucidate how these utilization trends affect outcomes across different groups. Functional and quality-of-life outcomes are not reported using these methods, so it is not possible to compare patients’ outcomes based on the surgery performed. Furthermore, patient presentation and mechanism of injury are not reported, preventing analysis of the indications for the surgeries performed. Another limitation of this study is the nature of the TriNetX database, which does not uniformly or reliably capture detailed clinical data to assess pre-op functional or socioeconomic status. The database is also updated live and may produce differing results if repeated. However, this database is a major strength of the study, as it allows large-scale analysis across several health centers, highlighting trends that may not have been elucidated at a smaller scale.
CONCLUSION
The hypothesis was upheld. Operative treatment for FNFx is approximately 85% arthroplasty and 15% ORIF. Specifically, THA utilization is increasing over time relative to HHA, suggesting a shift in surgeon preferences. Future studies should investigate the specific factors contributing to these dynamic trends in the utilization of these surgeries, as well as a closer scrutiny of surgical outcomes for THA versus HHA in displaced FNFx.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
No ethical approvals required for this work.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.