Introduction
CCOC, a histotype of epithelial ovarian cancer, accounts for 5-10% of all epithelial ovarian cancer cases in North America, with incidence ranging anywhere from 10-30% in East Asia, making CCOC a relatively rare pathology.1 However, endometriosis—a common condition in women of reproductive age—is considered a precancerous lesion of CCOC necessitating consistent monitoring if a patient is diagnosed with endometriosis.1 CCOC has a demonstrably poor prognosis with a high mortality rate in the two years following diagnosis.2 Contributing factors to a poor prognosis include lymphatic spread, platinum-based chemotherapy resistance, and late detection.3 Presentation of metastatic CCOC typically includes abdominal pain or ascites due to peritoneal involvement. This is due to tumor implantation on the omentum and abdominal organs.4,5 Initially presenting with vague musculoskeletal pain in the setting of metastatic CCOC is unusual, which raises questions about which symptoms to look for when considering CCOC as a differential diagnosis.
Case Presentation
A 66-year-old female with a past medical history significant for stage III CCOC, which was treated with chemotherapy and radical hysterectomy 10 years prior, presented to urgent care for diffuse left-sided musculoskeletal pain after a fall in her bathtub. X-rays showed no acute osseous abnormalities, but 25 cc of blood was aspirated from the knee. Bilateral knee injections and a left trochanteric bursa injection were given to reduce the patient’s pain. Physical therapy was also prescribed and alleviated her musculoskeletal pain, except for a persistent searing pain in her upper thigh. The patient’s pain was worse with activity and improved with rest and pain medication.
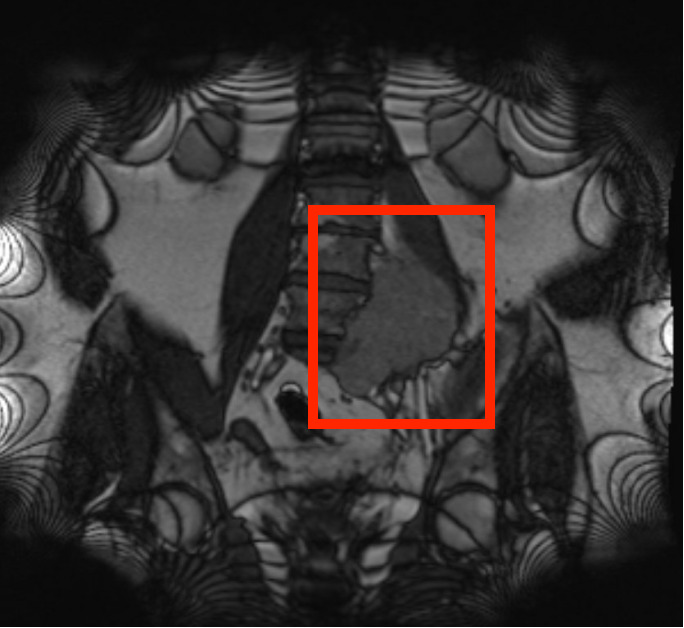
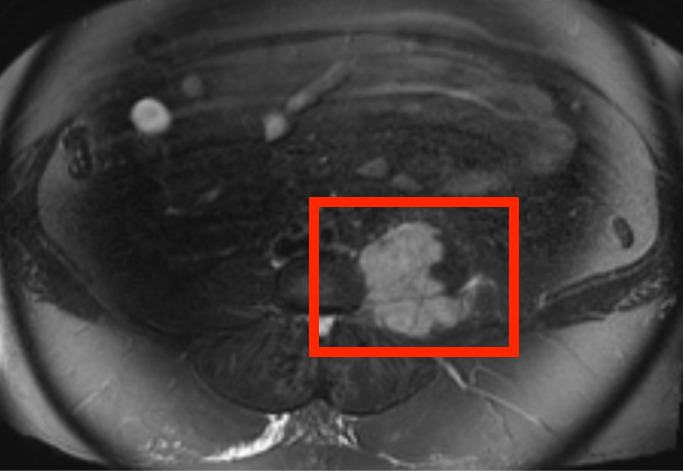
Additionally, the patient described the pain as continuous and achy, with no associated numbness or tingling. Interestingly, the patient denied any constitutional symptoms such as fevers, weight loss, or night sweats that would have raised a higher degree of suspicion for a recurrence of her previous cancer. This pain was thought to be chronic pain as it was first noted in her chart 4 months prior to her fall in the bathtub. Prior lumbosacral X-rays showed no acute abnormalities in the lumbosacral spine but demonstrated joint narrowing at L3-L4, prompting a magnetic resonance imaging (MRI) of the lumbar spine for suspected L3 radiculopathy. The MRI revealed a 6.7 cm left lumbosacral paravertebral mass with bone invasion of the L5 and S1 vertebral bodies and encasement of the L3-L5 nerve roots. [Figures 1 and 2]


Additionally, a computed tomography (CT) of the chest, abdomen, and pelvis demonstrated involvement of the left psoas muscle and left common iliac vessel. A CT-guided core biopsy of the prevertebral mass was positive for malignant cells consistent with metastatic clear cell carcinoma of Mullerian origin. Imaging indicated that external hemipelvectomy with a partial corpectomy of L4-L5 would be required to resect the mass. With these findings in mind, the orthopedic oncologist determined this mass to be extremely difficult to resect without significant morbidity. Although the choice to undergo a likely technically challenging case was presented to the patient, the surgical team and patient ultimately decided to proceed with palliative radiation. The patient subsequently received palliative radiation therapy with a significant reduction in size of the prevertebral mass on follow-up CT. The patient also reported resolution of left hip and thigh pain. Unfortunately, the patient sustained a C2 dens fracture during another fall about a month after completing radiation, which delayed her follow-up with gynecologic oncology. During this time, she underwent orthopedic procedures for her cervical fracture. The patient eventually followed up with oncology five months following her cervical orthopedic procedures, and a positron emission tomography (PET) scan at that time suggested recurrence of disease within her ascending colon. With the patient’s recent cervical spine procedures and new mesenteric mass, the oncology team and patient agreed to focus on improving her quality of life rather than aggressively treating her conditions. The patient has not been treated for her cancer in the last year and is still living with minimal pain while being observed by her oncology team.
Discussion
Epithelial ovarian cancer is the most lethal gynecologic malignancy. Inadequate screening strategies delay early detection, resulting in advanced disease at initial presentation. Treatment of advanced disease is much more challenging, necessitating early diagnosis for improved patient outcomes.6 CCOC—a histotype of epithelial ovarian cancer— is a rare malignancy that accounts for 5-25% of all ovarian cancers.1,6 Furthermore, CCOC metastasis is relatively uncommon (25-30%) due to screening techniques that can detect this histotype relatively early in disease progression.5,7 When metastasis does occur, symptoms are usually due to abdominal organ involvement. Peritoneal dissemination is most common, and symptoms generally include abdominal pain, abdominal distension, and malignant ascites. Additionally, direct invasion into abdominal and pelvic organs such as the uterus, fallopian tubes, and ovaries is common.5,7 CCOC lymph node metastasis is even less common, with about 10 patients presenting for metastasis out of a 205-patient cohort according to one study.6 Symptoms resulting from retroperitoneal nodal involvement do not typically develop until more advanced disease stages. These symptoms are usually related to mass effect and can manifest as lower back pain, abdominal pain, or radicular pain, as is the case with our patient.8
Due to the rarity of clear cell tumors and lymph node metastasis, pathologic diagnosis can be challenging. With this in mind, CCOC with atypical presentation may not be at the top of a clinician’s differential—and rightfully so. Not only is this condition poorly understood, but it is also exceedingly rare to be the perpetrator of thigh pain, given the plethora of other pathologies that must be considered first. For our patient, it is unfortunate that the retroperitoneal lymph node metastasis was diagnosed about 9 months after the patient’s initial presentation for upper thigh pain. Still, the rarity of the disease, compounded by the patient’s additional medical concerns, made diagnosis challenging. Retrospectively, obtaining an MRI when our patient initially presented with pain following a fall may have incidentally caught her retroperitoneal metastasis some months prior to her actual diagnosis, but this may not have altered the palliative care plan employed because these metastases usually take a long period of time to cause symptoms. Regardless, in a patient with a history of high-grade cancer, recurrence must be on the differential, irrespective of the likelihood of symptoms correlating to metastasis. Although our patient’s fall prompted a workup that incidentally found this patient’s cancer recurrence, her prior documented persistent searing leg pain refractory to conservative treatment should have raised a red flag in the eyes of her providers. Considering this, early screening with MRI may be warranted to detect these types of masses earlier in disease progression. With the development of more robust screening strategies, cases like our patient’s may be treated before surgical intervention becomes futile.
Conclusion
Metastatic CCOC is an uncommon condition with limited screening modalities, making effective treatment challenging. Despite these challenges, work is underway to develop screening strategies that can better detect the disease at an earlier stage, in hopes of preventing it from progressing past the point of no return.
Declaration of Conflict of Interest
The authors have no conflicts of interest to disclose relevant to this work.
Declaration of Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Ethical Approval of Study
This case report is exempt from IRB review as it does not constitute research involving human subjects per Cooper University Hospital IRB policy.
Declaration of Informed Consent
There is no information in the submitted manuscript that can be used to identify patients.