Introduction
Retrograde femoral intramedullary nail (rIMN) fixation in rodents has been applied in many orthopedic animal model studies, such as for fracture healing studies,1,2 biomechanical,3 genetic,4 and prosthetic joint infection studies (PJI).5 In rodent prosthesis models, retrograde femoral intramedullary nail fixation is a commonly used technique to simulate PJI in the tibiofemoral joint.6–8 A popular and established method to achieve rIMN fixation in rodent models involves an open medial parapatellar approach. To our knowledge, all published studies have described retrograde nailing using this open approach.6–8
Despite its popularity, the open medial parapatellar approach is a highly invasive procedure. Due to the extensive incision and significant disruption of the quadriceps-patellar complex (QPC) and joint capsule, this technique poses considerable challenges for preserving the integrity and anatomical arrangement of the native capsule, the tibiofemoral joint, and the patellofemoral and extensor mechanisms.6–8 In prosthetic joint infection models, the tissue damage caused by this technique significantly impairs the intra-articular delivery of bacteria or therapeutic agents to the tibiofemoral joint, primarily due to the extravasation of materials from the joint. As a result, there is a need for a minimally invasive retrograde femoral nailing technique that will minimize disruption to the native anatomy during retrograde femoral nail fixation and reduce the risk of extravasation of bacteria or therapeutic agents from the joint space. To that end, this study introduces a refined surgical approach that eliminates the need for extensive dissection of the quadriceps-patellar complex and joint capsule, thereby maintaining the physiological barriers and structural integrity of the joint. This technique could improve the translational relevance of rodent models used in orthopedic research by reducing invasiveness and preserving anatomical fidelity. Furthermore, it may offer greater consistency in intra-articular experimental delivery, enhancing reproducibility in studies focused on infection, healing, or drug delivery.
Methods
Our institution’s Institutional Animal Care and Use Committee (IACUC) approved the animal study protocol, and all procedures and experiments were conducted in accordance with the approved protocol and institutional guidelines. Additionally, we adhered to the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines and have included the ARRIVE checklist.
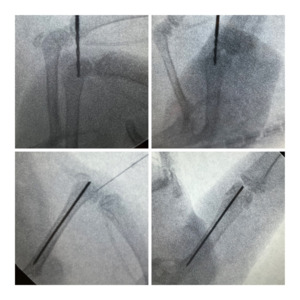
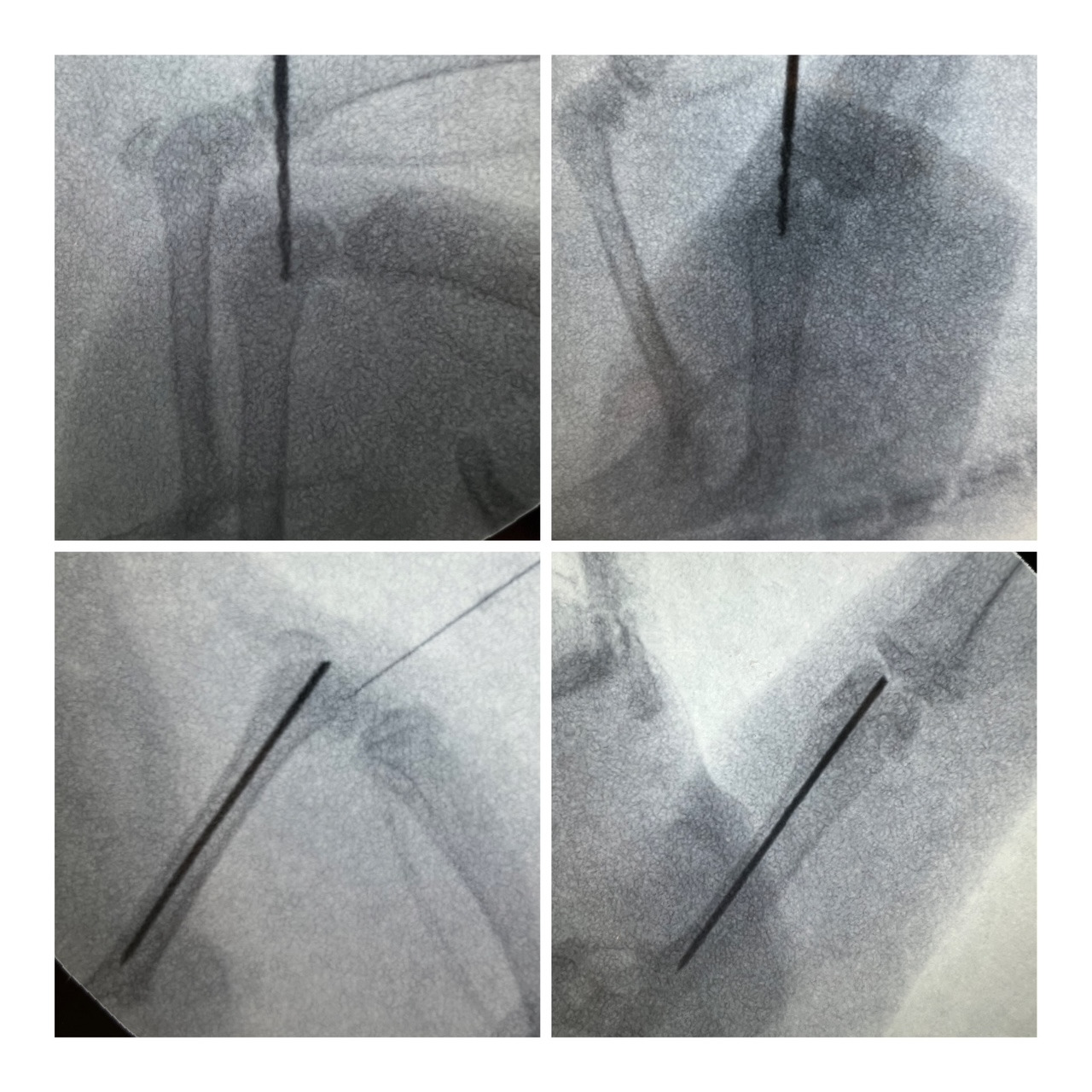
The surgical technique was performed on 48 skeletally mature male Sprague-Dawley rats (Charles River Laboratories, Wilmington, MA) aged 13 weeks. Prior to the procedure, the rats were allowed a minimum of 48 hours of acclimation. The procedures were conducted on a water-circulating warming pad. Anesthesia was administered via inhalation using 2% isoflurane with oxygen (2L/min). Preoperatively, analgesia was administered via subcutaneous injection of 1 mg/kg of 1% sustained-release buprenorphine. The limb was shaved with an electric shaver and prepared with 1% povidone solution, followed by a 70% ethanol solution. The operative extremity was placed through a fenestrated surgical drape. A 1 cm longitudinal parapatellar skin incision was made on the right hind leg. Subsequently, a 2 mm longitudinal incision was made along the patellar tendon just inferior to the inferior pole of the patella. Using mini C-arm fluoroscopic guidance, a 1.2 mm drill bit was manually advanced through the opening in the patellar tendon and subsequently through the cortical bone of the intercondylar notch. The femoral canal was reamed manually using the drill bit under fluoroscopic guidance. A 0.8 mm stainless steel Kirschner wire (K-wire) (GreatLH Orthopedics, Chandu, China) was advanced manually through the start point of the intercondylar notch using the hole produced by the 1.2 mm drill bit and into the reamed femoral medullary cavity until it engaged the proximal cortical bone of the femur. Intraoperative fluoroscopic imaging confirmed the placement of the K-wire [Figure 1].
The K-wire was cut to leave a 1 mm protrusion into the joint space. A single 4-0 nylon suture was used to close the patellar tendon. The skin was closed appropriately using 4-0 nylon sutures. The rats were given soft dressings. The animals were then transported to a postoperative recovery area, where they recuperated under a heat lamp. Observations of the rat’s right leg weight-bearing capacity, overall activity, feeding behavior, and any signs of bleeding were conducted at 1, 3, 4, and 5 days following the surgical procedure. The animals were provided with environmental enrichment in their cages.
The rats were euthanized at an interval of five to seven days postoperatively, and the integrity of the capsule of each rat was assessed by an orthopedic surgeon/postdoctoral fellow (MJS) during a post-mortem cadaveric study. Immediately following euthanasia, blood samples were obtained via cardiac puncture, while joint fluid and periarticular tissues were collected through surgical tissue harvesting. To assess for potential infection, joint fluid, periarticular tissues, and blood samples from all experimental subjects were cultured using brain heart infusion (BHI) broth (AG Scientific Inc., San Diego, CA, USA).
In a previous rat model of septic arthritis, favorable outcomes were achieved using a modified retrograde nailing technique, which led to the development of the novel surgical approach described in this study.5
A video of the procedure is available upon request.
Results
The weights of the rats varied from 329 to 560 grams, with a mean weight of 432.5 ± 52.5 grams. The time required to complete the femoral nail fixation procedures, from start to skin closure, ranged from 6 to 90 minutes, with an average of 20.3 ± 15.3 minutes. Notably, the 90-minute procedure represented a significant outlier, as the second-longest operative time was 50 minutes. The extended duration of the 90-minute surgery was attributable to intraoperative breakage of the K-wire within the femoral tunnel, which necessitated additional surgical time for management. The interquartile range (IQR) for the duration of the procedures was calculated as follows: the first quartile (Q1) was 10 minutes, the median (Q2) was 13 minutes, and the third quartile (Q3) was 30 minutes. Mean surgical time was also higher for the first 10 animals (40.1 minutes) than for the subsequent 38 animals (14.9 minutes; t-test, t=6.0, p<0.0001).

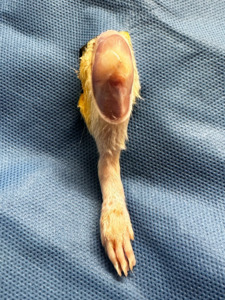
Of 48 rat subjects, 47 (98%) maintained complete capsular integrity and preserved the patellar tendon and articular capsule at 5 days postoperatively [Figure 2], as assessed by a second orthopedic surgeon under loupe magnification. All rats (48/48, 100%) were ambulatory postoperatively. In the evaluation for potential infection, no bacterial organisms were isolated from the blood, joint fluid, or periarticular tissues in any of the rats. The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Discussion
Here, we describe a novel method for retrograde intramedullary nailing in a rat model that achieves a short operative time and a rapid learning curve while maintaining the rat knee’s capsular integrity and the animal’s ambulatory status.
Our technique offers multiple advantages over traditional, open-nailing methods. First, the complete preservation of the joint capsule and the patellar tendon is based on post-mortem direct visualization in 98% of the cases, underscoring the repeatability and efficacy of this technique. To our knowledge, no studies have evaluated the integrity of the joint capsule with a second-look following surgery. This technique ensures precise and reliable drug delivery into the joint space for intra-articular injections and minimizes invasive injury to surrounding structures. Additionally, using fluoroscopic guidance to confirm K-Wire entry into the femoral canal maintains the technique’s accuracy while minimizing damage to the joint space or surrounding tissues. This technique is useful in translational research, providing a more consistent and reliable method for modeling prosthetic joint infections (PJI) and conducting medication-related murine trials.
Articles describing the conventional surgical method through a medial parapatellar incision do not address the repair of the parapatellar retinaculum.1,9 Repairing and suturing the parapatellar retinaculum can be more challenging and less dependable than patellar tendon repair due to differences in tissue properties. However, based on our experience, we found the repair of the parapatellar retinaculum with simple nylon sutures to be both convenient and reliable.
The average surgical duration of 20.3 minutes (14.9 minutes if accounting for the “learning curve” of the first 10 animals) highlights its efficiency and speed compared to traditional methods. There is a paucity of data on surgical durations with conventional methods; however, our approach yields surgical times comparable to those reported in previous studies, including the current practice of the open medial parapatellar approach, as documented by Bonnarens et al.10
In 2000, Bhandari et al.11 reported a percutaneous technique of femoral nailing, employing a similar retrograde method of pin insertion through the trochanteric fossa distal to the femoral condyle. While they reported satisfactory results and a short procedure time, this technique requires skin contact with the implant, risking contamination of the implant with skin flora. Although our technique involves a slightly longer duration than this percutaneous method, it minimizes contact between the animal skin and the implant while also allowing accurate concurrent intra-articular knee injections, which is especially useful in models of periprosthetic infection.
This study has several limitations. The most significant is the absence of a control group utilizing a conventional technique for comparison. Second, all procedures were performed by a single orthopedic surgeon, which may limit generalizability; inclusion of multiple surgeons could have enhanced the external validity of operative time and outcome assessments. Additionally, the lack of histologic and biomechanical evaluations is an important limitation, particularly for assessing capsular integrity. Finally, no postoperative functional or behavioral assessments were performed in the rat model. The absence of gait analysis, weight-bearing measurements, or other validated rodent functional outcome measures limits the interpretation of the in vivo clinical significance of the findings.
In conclusion, we report an efficient, less-invasive technique for retrograde pin insertion under fluoroscopy. This technique preserves capsular integrity and native anatomical structures during retrograde intramedullary nailing, thereby significantly reducing the risk of contamination and subsequent infection. It has broad applicability in translational science, particularly for modeling orthopedic fracture fixation and prosthetic joint infections.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The Darwin Project partly funded this study (Grant ID 65646).
Declaration of ethical approval for study
The Institutional Animal Care and Use Committee approved the animal study protocol at the Beth Israel Deaconess Medical Center (Protocol #038-2023, approved 16 January 2024). All the animal-based procedures and experiments were conducted in accordance with institutional guidelines and the approved protocol.
Declaration of informed consent
Not applicable
Data Availability
The data supporting this study’s findings are available from the corresponding author upon reasonable request.