INTRODUCTION
Low-velocity gunshot wounds (GSWs) to the pelvis constitute a distinct subset of ballistic trauma characterized by heterogeneous injury patterns involving the pelvic ring, acetabulum, and adjacent soft tissues. These injuries are frequently accompanied by damage to the gastrointestinal, genitourinary, or vascular systems, each of which introduces distinct contamination pathways influencing orthopaedic management.1,2 The diagnostic and therapeutic complexity of these cases necessitates individualized, multidisciplinary decision-making to minimize morbidity and optimize outcomes.
Prophylactic antibiotic administration is widely accepted as an initial component of management, particularly in the presence of open fractures or suspected hollow viscus injury. Surgical intervention, including debridement, washout, and fixation, may be indicated based on fracture stability, degree of contamination, and patient physiology. However, substantial variability persists regarding the timing and extent of operative management, especially in hemodynamically stable patients with low-velocity injuries.
Infectious complications, deep tissue morbidity, and overall functional outcomes remain critical endpoints when evaluating treatment strategies. With firearm-related pelvic trauma increasing in many urban centers and the estimated annual economic burden exceeding $16 billion, refinement of evidence-based management pathways is imperative.3–8 This Current Concepts Review summarizes the contemporary literature on antibiotic use and surgical management in low-velocity ballistic pelvic fractures, with particular emphasis on infection risk and complication profiles, to inform clinical decision-making and identify priorities for future research.
REVIEW
Initial Multidisciplinary Evaluation and Diagnostic Workup
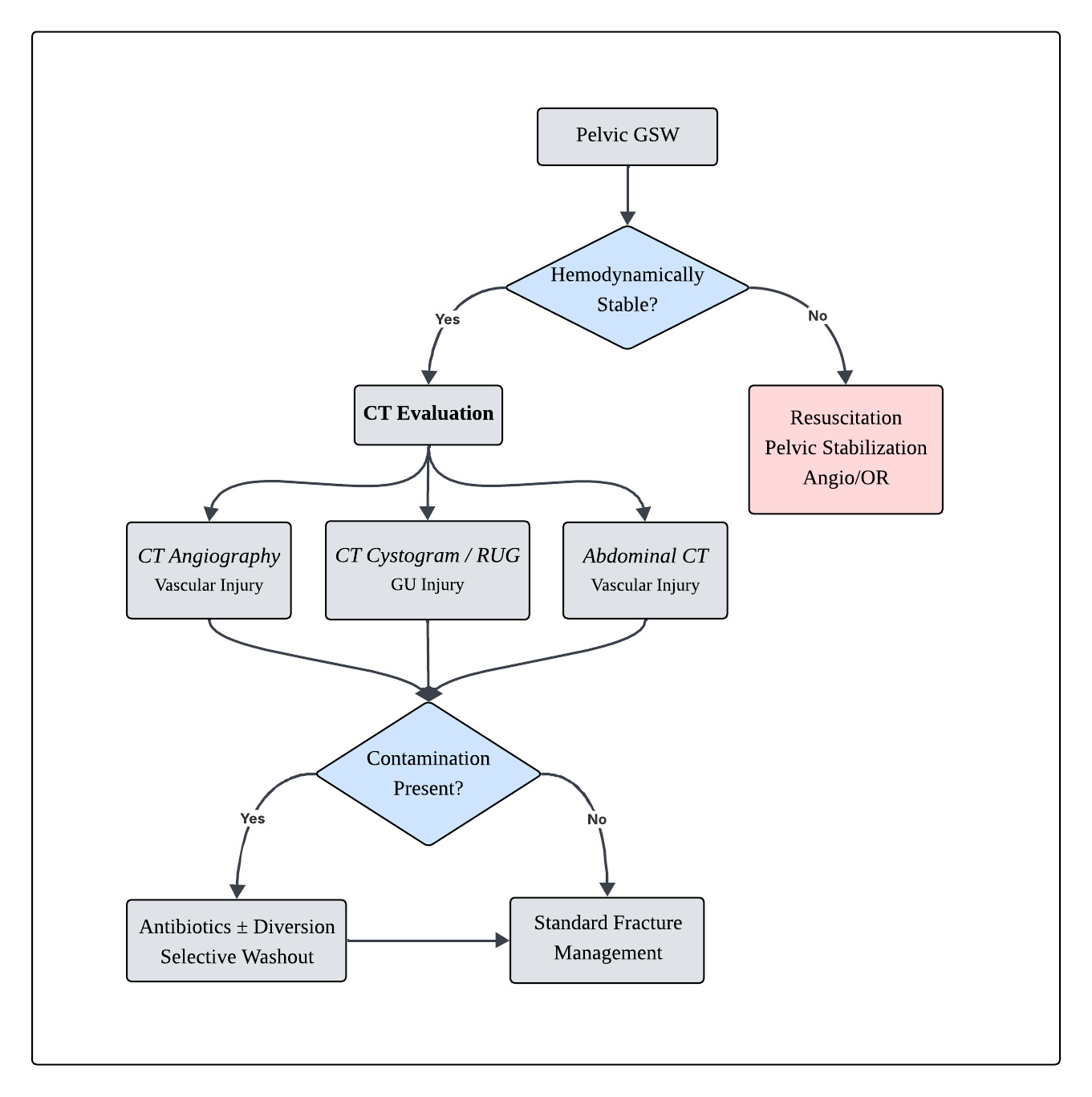
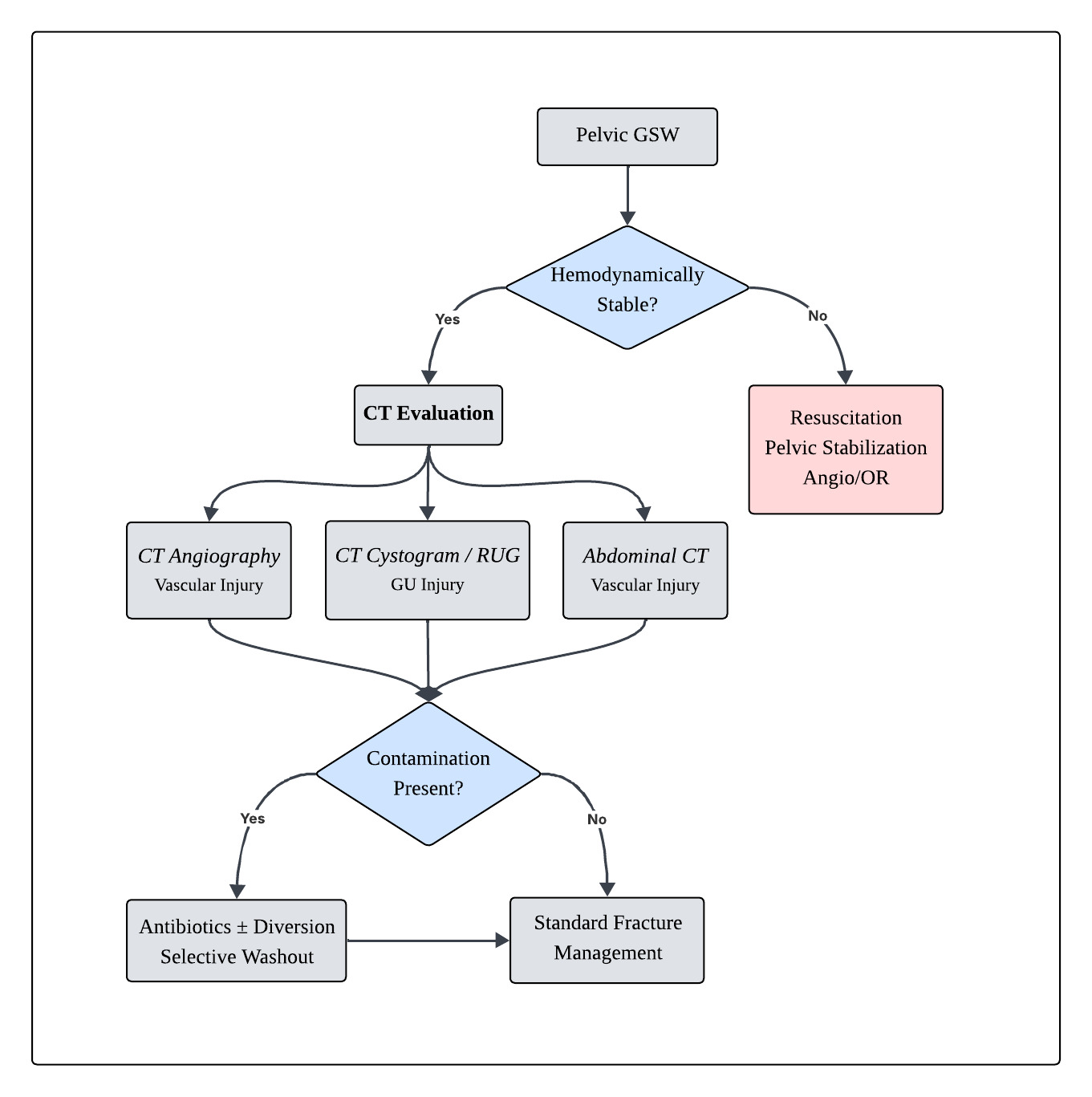
Initial management of ballistic pelvic fractures centers on rapid multidisciplinary assessment to identify associated visceral or vascular injuries, as these findings directly influence orthopaedic decision-making. Hemodynamic stability remains the primary determinant of early evaluation. Unstable patients require immediate hemorrhage control following Advanced Trauma Life Support principles, including pelvic stabilization, resuscitation, and consideration of angioembolization or operative exploration.9,10
In hemodynamically stable patients, contrast-enhanced computed tomography (CT) serves as the cornerstone of evaluation. CT angiography is recommended when vascular injury is suspected based on trajectory, expanding hematoma, or contrast extravasation.9 Assessment of genitourinary injury includes CT cystography for suspected bladder injury and retrograde urethrography when urethral disruption is suspected, particularly in the presence of blood at the urethral meatus or inability to void.11,12
Evaluation for hollow viscus injury relies on trajectory analysis and CT imaging findings such as free air, bowel wall thickening, or mesenteric injury. In equivocal cases, diagnostic laparoscopy or exploratory laparotomy may be required to establish the status of contamination.13 Early identification of bowel or urinary contamination is critical, as these findings guide antibiotic selection, the need for diversion procedures, and the timing of orthopedic intervention.
Accordingly, management of low-velocity ballistic pelvic fractures proceeds through a structured decision pathway integrating physiologic status, injury trajectory, and associated organ injury, allowing stratification into operative versus nonoperative orthopaedic treatment strategies. [Figure 1, Table 1]
Antibiotic Management
Injury to the gastrointestinal tract and subsequent contamination are the strongest predictors of infectious orthopedic complications in ballistic pelvic fractures.14,15 As such, antibiotic prophylaxis remains a cornerstone of management. Multiple studies, including those by Nguyen et al. and Marecek et al., have demonstrated that antibiotic administration in low-velocity ballistic fractures is both common and effective in limiting infection.16,17
Despite widespread use, no standardized protocol exists regarding antibiotic selection or duration. A systematic review by Dehne et al. concluded that short-course antibiotic prophylaxis (≤48-72 hours) is sufficient following abdominal ballistic injuries.18 Nguyen et al. similarly reported no significant difference in infection rates between single-dose and multidose regimens (12.5% vs 14.6%, respectively; p = 1.00).19 Shorter courses (1-3 days) were not associated with higher rates of osteomyelitis, meningitis, Clostridioides difficile infection, or multidrug-resistant organisms, and resulted in comparable lengths of hospital stay.18
Antibiotic selection should be tailored to injury characteristics. In the absence of bowel injury, broad-spectrum intravenous agents, such as penicillin, first-generation cephalosporins, or aminoglycosides, administered for 1-3 days are generally recommended.20,21 In patients requiring operative intervention for gastrointestinal or significant soft-tissue injury, third-generation cephalosporins are commonly advocated for a similar duration.20–22 Adjunctive measures, including tetanus prophylaxis, should be considered on a case-by-case basis.
Operative Management
Fracture Fixation
Indications for orthopedic fixation are primarily dictated by fracture stability. Based on Young-Burgess and Tile classification systems, most low-velocity ballistic pelvic fractures are mechanically stable, as they typically spare the pelvic ligaments and floor.23 Consistent with this observation, published series report a low incidence of fractures requiring operative stabilization, with fixation most often reserved for select acetabular injuries.1,3,21,24
Debridement & Washout
The role of routine debridement and washout in preventing infection remains controversial. Shannon et al. reported a significantly lower infection rate among patients undergoing irrigation and debridement compared with those managed nonoperatively (8% vs 46%; p < 0.05), independent of fecal contamination.25 In contrast, Nguyen et al. found no protective benefit from surgical debridement, reporting similar infection rates between nonoperative antibiotic management (3.8%) and operative intervention (3.6%).16
Other studies suggest that aggressive surgical debridement may increase the risk of infection. Watters et al. observed comparable infection rates between patients who underwent debridement and those who did not (7% vs 6%).13 In comparison, Sathiyakumar et al. demonstrated substantially higher infection rates with extensive debridement compared with superficial or no debridement (20.8% vs 2.9%).22
Consensus emerges for selective debridement in cases involving intra-articular penetration, extensive soft-tissue destruction, vascular injury, or high-velocity mechanisms.10,24 Therefore, differentiation between high- and low-velocity injuries is a critical initial step in determining the appropriateness of surgical washout.
Fecal Diversion
Fecal diversion has historically been employed to reduce infection in open pelvic fractures, including ballistic injuries. However, contemporary data suggest limited benefit in isolated low-velocity ballistic pelvic fractures. Woods et al. reported no reduction in abdominopelvic infectious complications with diversion, although a potential benefit was noted in patients with extensive soft-tissue injury or posterior wounds.26 Evidence from penetrating colorectal trauma similarly supports a selective approach, demonstrating comparable infectious outcomes between diverted and non-diverted patients when injuries are appropriately managed with debridement, antibiotic therapy, and source control.27 These findings suggest that, in low-velocity ballistic pelvic fractures, fecal diversion should be individualized based on injury severity, degree of contamination, and physiologic status rather than employed routinely.
Genitourinary Injury
Genitourinary (GU) injury frequently accompanies ballistic pelvic trauma and represents an underrecognized contributor to deep pelvic infection. Bladder and urethral injuries may result in urinary extravasation into the pelvic soft tissues, creating a contaminated environment that increases the risk of osteomyelitis, hardware colonization, and wound complications.10,28
Evaluation of suspected GU injury is typically guided by mechanism and clinical findings, with CT cystography recommended for suspected bladder injury and retrograde urethrography performed when urethral disruption is suspected, particularly in the presence of blood at the urethral meatus, pelvic fracture displacement, or inability to void.11 Early identification is critical, as unrecognized urine leakage may mimic or compound infection traditionally attributed to bowel contamination.
The urinary diversion strategy depends on the injury pattern. Foley catheter drainage is generally sufficient for uncomplicated extraperitoneal bladder injuries, whereas suprapubic catheter placement is preferred in cases of urethral injury, complex bladder disruption, or when prolonged diversion is anticipated.11,12 From an orthopaedic perspective, gross urinary contamination alone does not universally mandate formal fracture debridement or washout; however, operative irrigation may be considered when significant extravasation coexists with open fractures, retained foreign material, or planned internal fixation. Management should therefore be individualized through multidisciplinary coordination between trauma, urology, and orthopaedic teams.
Removal of Retained Bullets
There is broad agreement regarding indications for bullet removal. Retained extra-articular bullets confer minimal infectious risk, even in the presence of bowel injury, and do not routinely require extraction.10,20,21,23,24,29
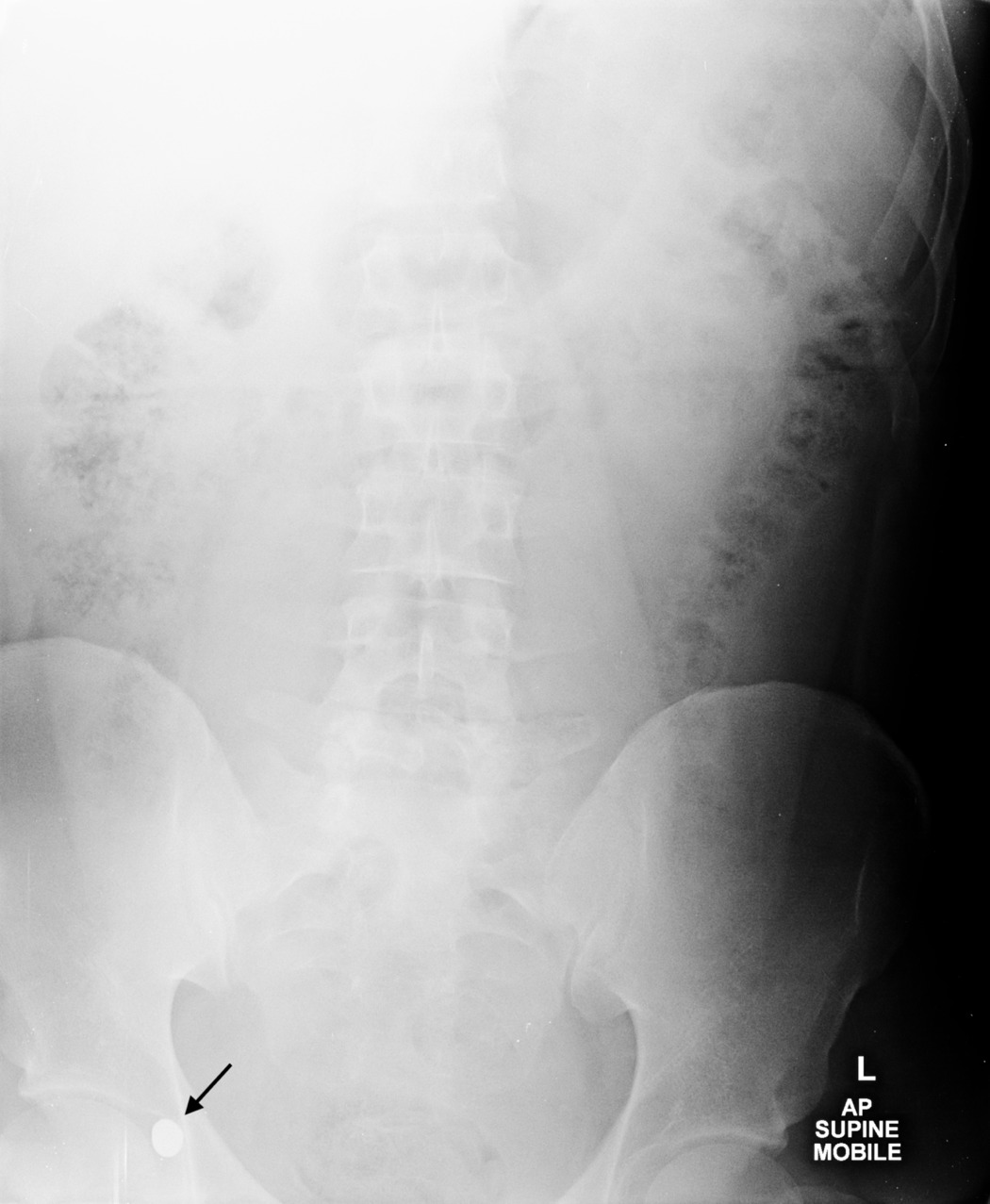
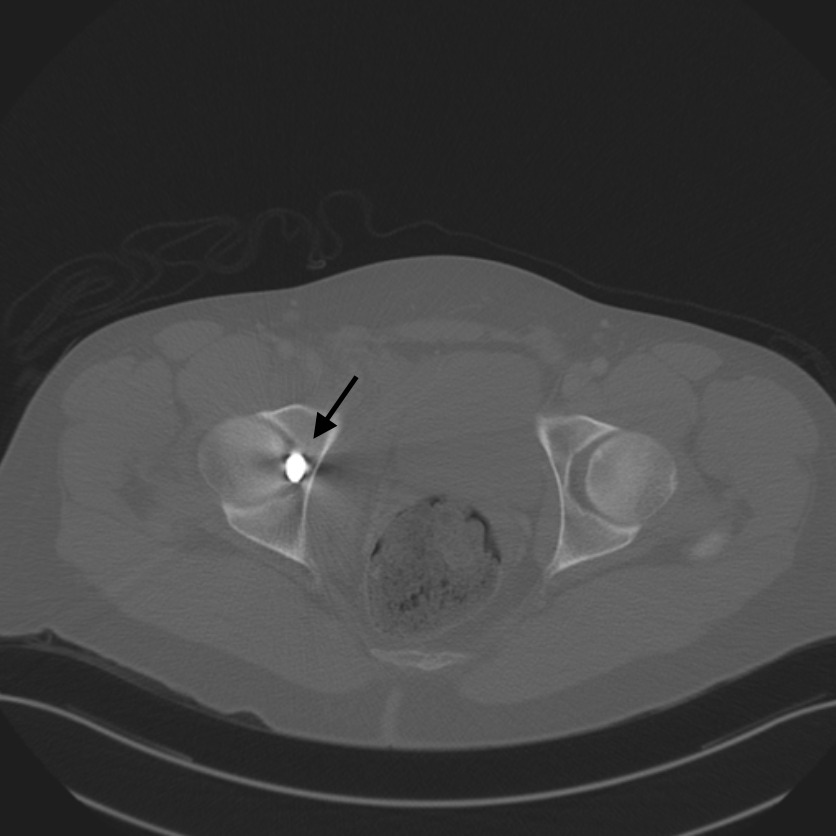
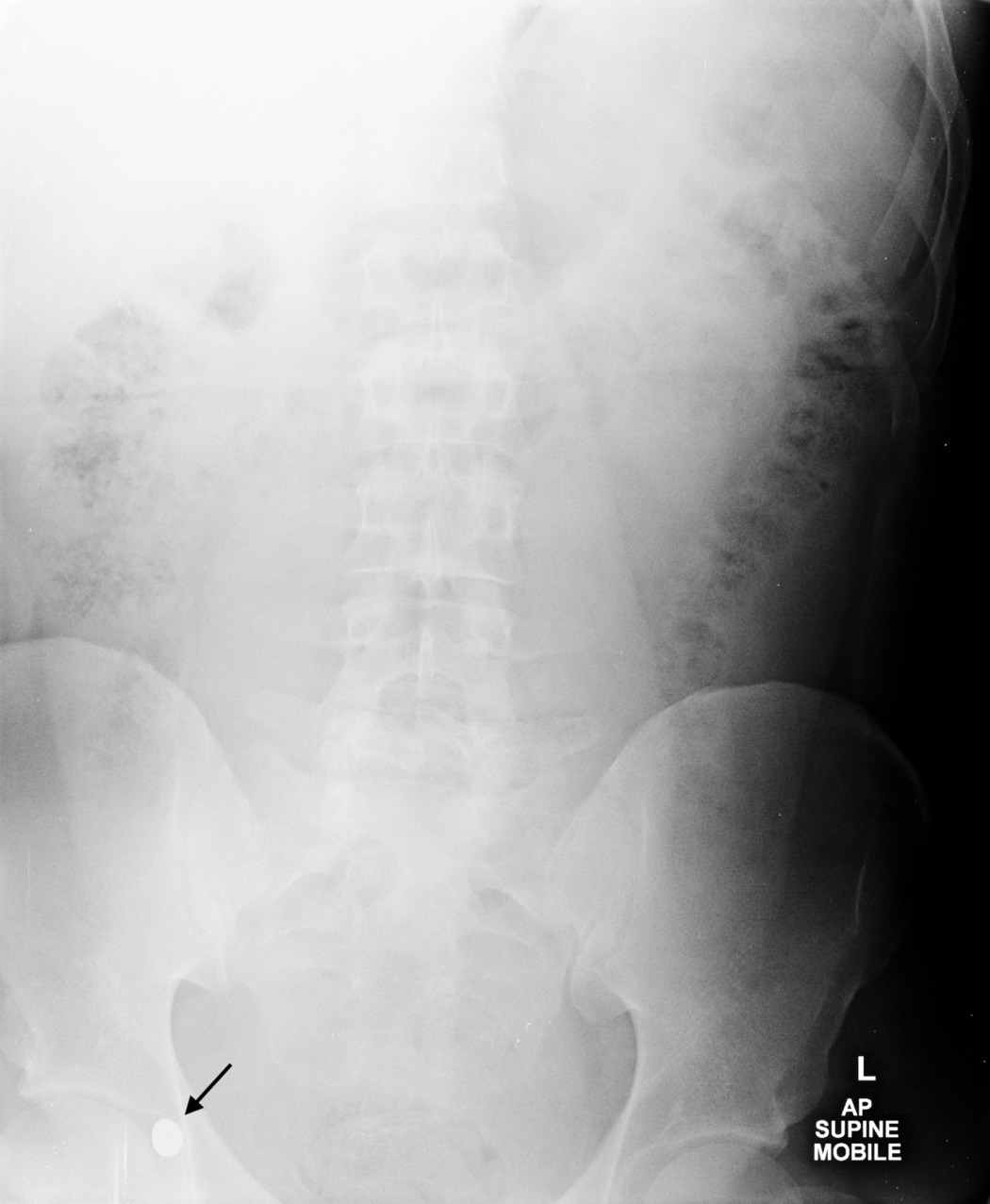
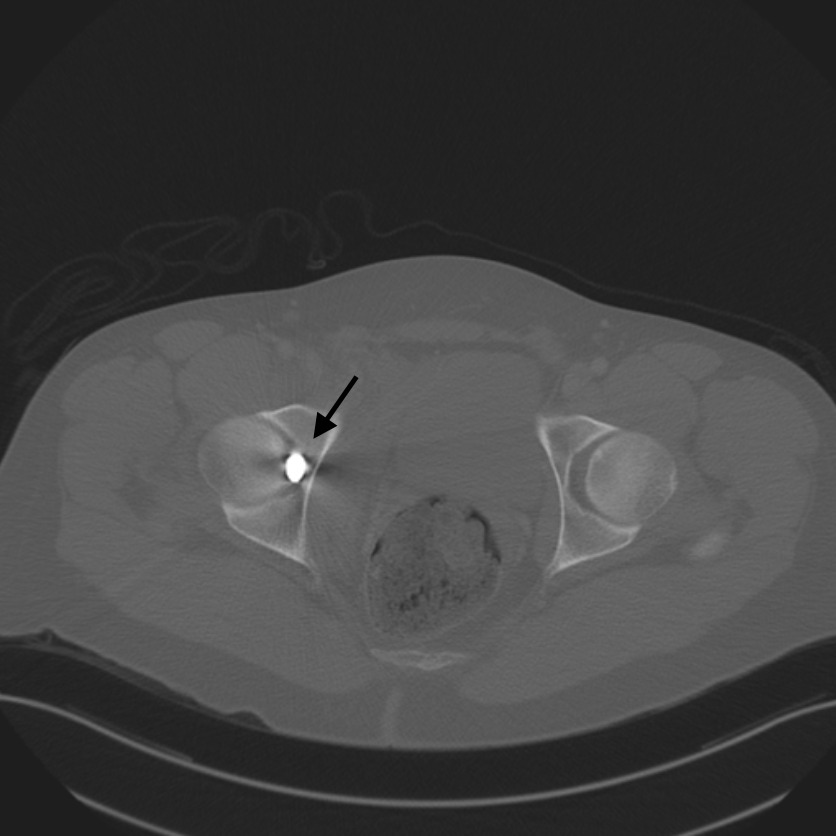
In contrast, intra-articular bullets should be removed to prevent lead toxicity. Radiographic identification of intra-articular projectile fragments is essential for operative planning. An example of a retained intra-articular bullet is demonstrated on an AP pelvis radiograph [Figure 2], with axial CT imaging confirming intra-articular localization within the acetabulum [Figure 3].
Beyond systemic toxicity, retained intra-articular projectiles may cause substantial mechanical damage to the joint. Metallic fragments function as third-body abrasive particles within the synovial environment, accelerating articular cartilage wear and promoting rapid degenerative joint changes. Repetitive joint motion facilitates fragmentation and dispersion of metallic debris, resulting in synovitis, chondrolysis, and early post-traumatic osteoarthritis, particularly in weight-bearing articulations such as the hip. Accordingly, intra-articular bullet retention represents not only a toxicologic concern but also a distinct orthopaedic indication for prompt surgical removal to preserve joint integrity and long-term function.2,30–33 Surgical approach depends on surgeon expertise, joint involvement, and associated intra-articular pathology, with both arthroscopic and open techniques described.2,3,20
Complications
Ballistic pelvic fractures are associated with a higher complication burden than extremity ballistic injuries. While extremity GSWs carry infection rates of approximately 1.8%-3%,13,21,22 pelvic involvement substantially increases risk due to bowel penetration and fecal contamination.16,19 Systematic reviews report infection rates of 21%-40% in ballistic pelvic fractures with bowel injury, compared with markedly lower rates in the absence of visceral involvement.14,22,34 This increased morbidity is accompanied by higher mortality, with pelvic ballistic trauma demonstrating a 32% relative increase compared with extremity injuries (10.6% vs 8%).35
Retained intra-articular lead projectiles may result in plumbism, as lead becomes solubilized in synovial fluid and systemically absorbed. Clinical manifestations include anemia, abdominal pain, nephropathy, encephalopathy, neuropathy, and degenerative arthritis.31
Hemorrhage and shock represent additional life-threatening complications. Although most pelvic bleeding is venous, arterial injury occurs in 10%-20% of cases and is associated with severe hemodynamic instability and increased mortality.9
Limitations
The existing literature on ballistic pelvic fracture management is constrained by the predominance of lower-level evidence studies. A majority of the existing literature consists of level III-IV studies, including case series and retrospective reviews, which inherently possess limitations in their ability to establish definitive treatment protocols. The reliance on lower levels of evidence contributes to practice variability and the absence of a standardized management. The absence of randomized controlled trials and large prospective cohorts underscores the need for higher-quality evidence to establish standardized, evidence-based treatment algorithms.
CONCLUSION
Low-velocity ballistic pelvic fractures pose unique infection-related and management challenges. Current evidence supports short-course, broad-spectrum antibiotic prophylaxis tailored to the presence or absence of bowel injury. Routine aggressive surgical debridement and fecal diversion do not consistently reduce infection rates and should be reserved for clearly defined indications, such as fracture instability. Bullet removal is indicated for intra-articular retention to prevent lead toxicity, while extra-articular bullets may be safely observed. Given the predominance of low-level evidence, well-designed prospective studies are urgently needed to define optimal, standardized management strategies and improve outcomes in this complex patient population.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest related to the content presented in this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval
Institutional Review Board approval was not required for the production of this manuscript.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs/images) in the submitted manuscript that can be used to identify any patients.