INTRODUCTION
Olecranon fractures are common elbow injuries, accounting for approximately 10% of all upper-extremity fractures. The most frequent pattern, representing up to 90% of cases, is a transverse or simple oblique fracture with no comminution and a stable elbow joint (Mayo Type 2A).1 These injuries most commonly occur following a fall onto a flexed elbow, either from a direct impact or as an eccentric loading triceps avulsion-type fracture.2
For displaced fractures, operative fixation is typically indicated and most commonly performed using stainless-steel tension band wiring (TBW) or plate-and-screw constructs. Although these techniques reliably achieve fracture union, they are associated with high rates of hardware removal (12–82%) due to symptomatic hardware, hardware loosening or migration, and wound complications.1,3–6 Such complications are not completely unexpected given the thin soft-tissue envelope over the proximal ulna and that the posterior elbow frequently bears weight during activities of daily living.
To reduce hardware prominence and associated complications, alternative fixation strategies have been explored, including hybrid screw and wire constructs, dual plating with smaller-sized plates on the lateral olecranon surfaces, intramedullary screws/nails, and suture anchor constructs. A recently described technique utilizes high-tensile-strength, second-generation orthopedic sutures to create dual tension band constructs, with generally favorable clinical outcomes reported in the literature.2,7 Notably, none of these clinical case series reported a need for postoperative hardware removal or significant hardware-related soft tissue complications.
However, concerns remain that suture-based fixation may not provide the same mechanical robustness as traditional metal wire constructs or plate fixation. To address this concern, four recent biomechanical studies have demonstrated equivalent or improved strength of suture constructs compared with TBW.8–11 Nevertheless, clinical series have still reported instances of loss of reduction, fracture separation, delayed union, and nonunion, which may reflect limited absolute stability provided by some suture-based constructs.5
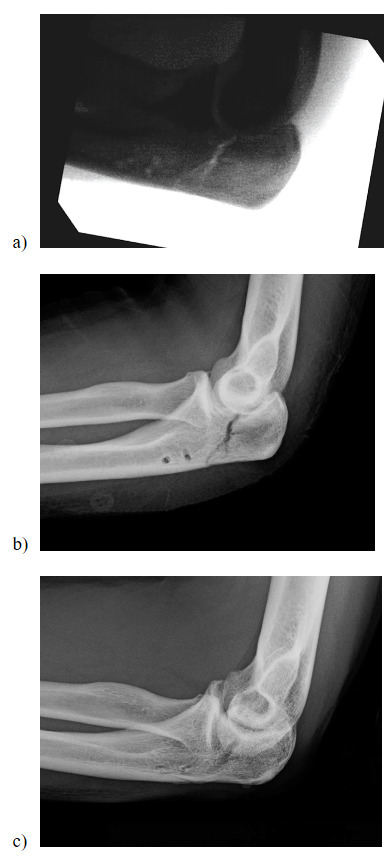
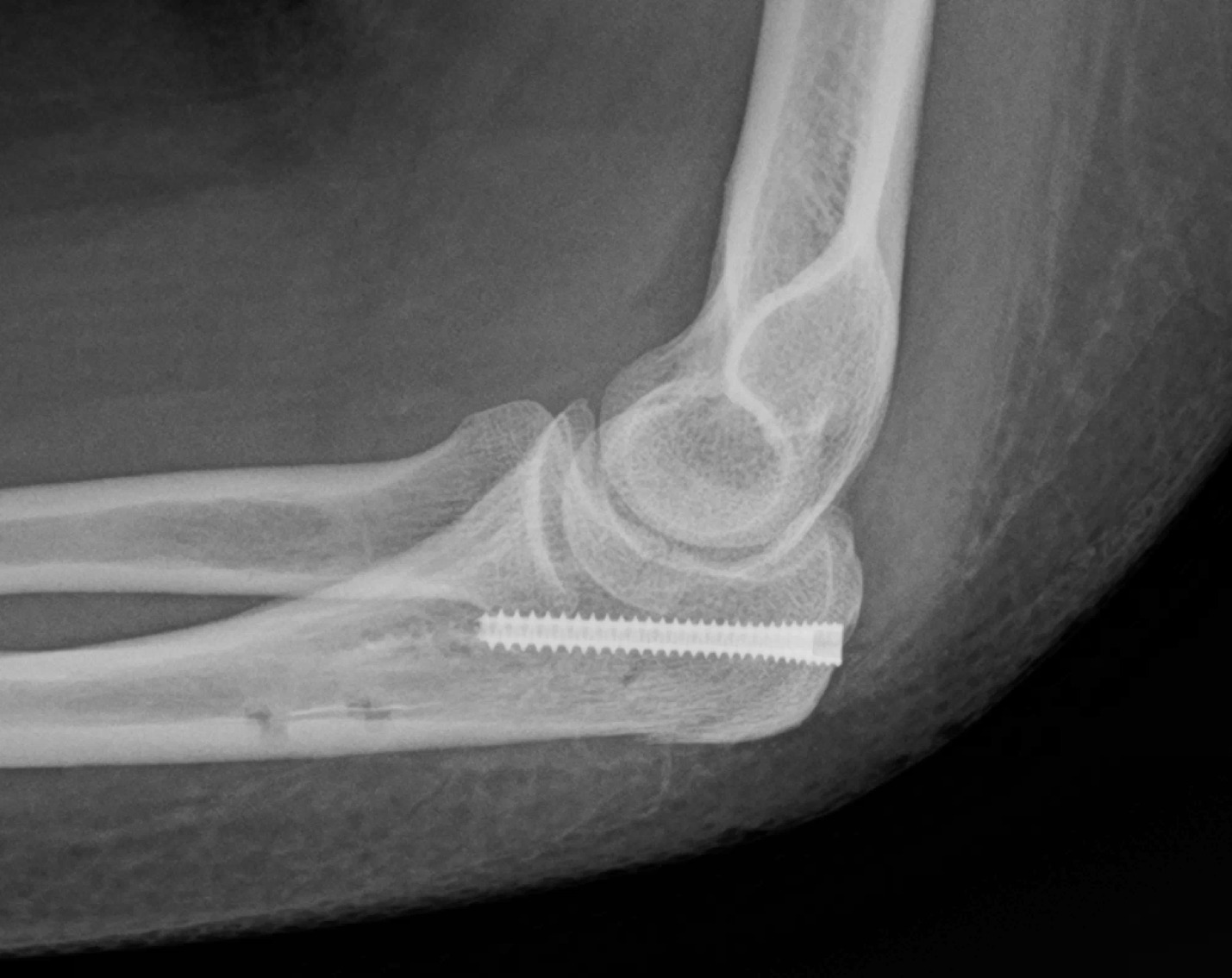
In 2019, we adopted the all-suture dual tension band technique (STB) described by Phadnis and Watts for the treatment of Mayo type 2A olecranon fractures.2 Consistent with their clinical results and subsequently published reports from other authors, we observed no issues related to hardware prominence, wound healing, or the need for hardware removal. We found the STB functional outcomes to be excellent and comparable to those reported with traditional fixation techniques. However, in several patients, early postoperative radiographs demonstrated subtle fracture gapping of a few millimeters, raising concern for inadequate or loss of fixation. All gapped fractures ultimately healed well except for one fracture that progressed to nonunion, requiring revision open reduction and internal fixation with plate-and-screw fixation. [Figure 1]
_immediate_postoperative_fluoroscopy_image__b)_radiograph_in_the_office_at_2_weeks_post_.png)
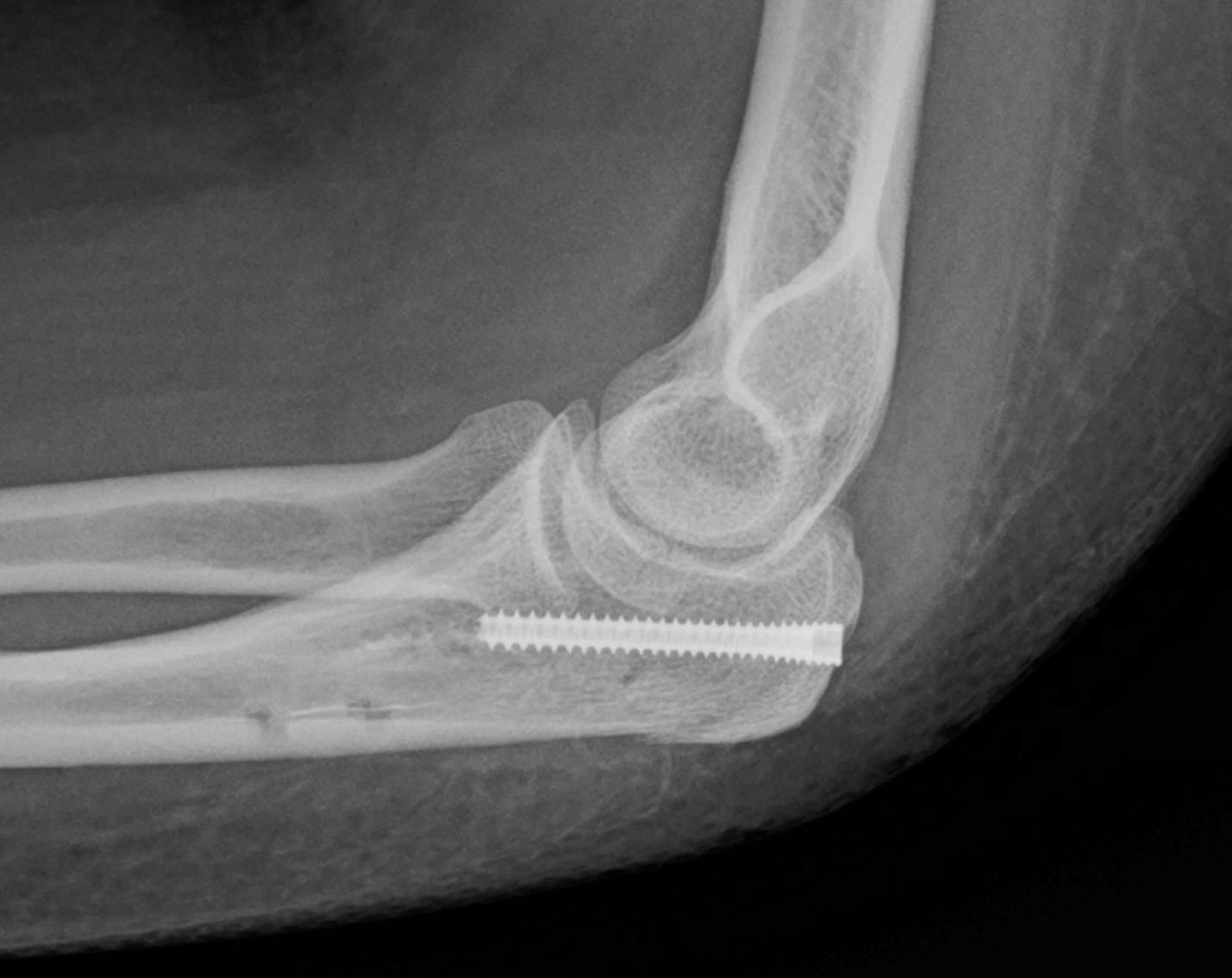
Following this complication, we modified the STB construct by adding a headless compression screw (HCS) in a “belt-and-suspenders” strategy to provide additional fracture compression and resist lateral translation and fracture gapping. [Figure 2] A retrospective review of the subsequent 11 patients treated with the modified suture tension band (MSTB) technique demonstrated no postoperative fracture gapping, and all fractures healed uneventfully (results pending publication). We concluded that the HCS was instrumental in resisting fracture gapping and reducing the risk of non-union. Based on these promising radiographic outcomes, we have adopted the MSTB for all Mayo 2 olecranon fractures and have been encouraged by the clinical outcomes. The following section describes the MSTB surgical technique.
INDICATIONS
This technique is indicated for transverse or short oblique olecranon fractures with no comminution and a stable elbow joint (Mayo type 2A). It is particularly well-suited for very proximal olecranon fractures, where plate fixation can be technically challenging. Because of the minimal hardware profile, this technique may also be advantageous in patients with small skeletal anatomy or thin or compromised posterior elbow soft tissues, where traditional metal implants may be more problematic.
CONTRAINDICATIONS
Given that this technique functions as a tension band construct that relies on compression at the fracture site for stability, fractures with more than minimal comminution are contraindicated. Additional contraindications include fractures associated with ulnotrochlear instability (Mayo type 3), fractures distal to the bare area of the olecranon, distal oblique fracture patterns, fractures with substantial articular depression, and fractures involving the coronoid process. These injury patterns generally require plate-and-screw fixation to achieve adequate stability and anatomic reduction. Other factors that may preclude the use of this technique include open fractures and patients with poor soft-tissue coverage.
SURGICAL TECHNIQUE
Patient Positioning
The patient may be positioned either supine or in the lateral decubitus position. Our preference, which allows excellent access to the fracture and facilitates intraoperative imaging, is the supine position with the operative arm draped over the body and supported by several stacked blankets on the chest. With this configuration, an assistant is typically required to help control the arm during the procedure. For fluoroscopic imaging, a mini C-arm is brought in from the operative side of the patient. The patient’s arm can be lifted from the blanket stack and positioned on the image intensifier, which is pushed in to abut the side of the operative table. It is helpful to position the patient on the very edge of the operative table to facilitate fluoroscopic imaging.
The procedure is usually performed with an upper-arm tourniquet. However, it can also be performed using the wide-awake local anesthesia no-tourniquet (WALANT) technique. For WALANT procedures, we recommend injecting at least 40 mL of 1% lidocaine with epinephrine at the surgical site and waiting a minimum of 30 minutes prior to incision to ensure adequate anesthesia and hemostasis.
#Surgical Technique
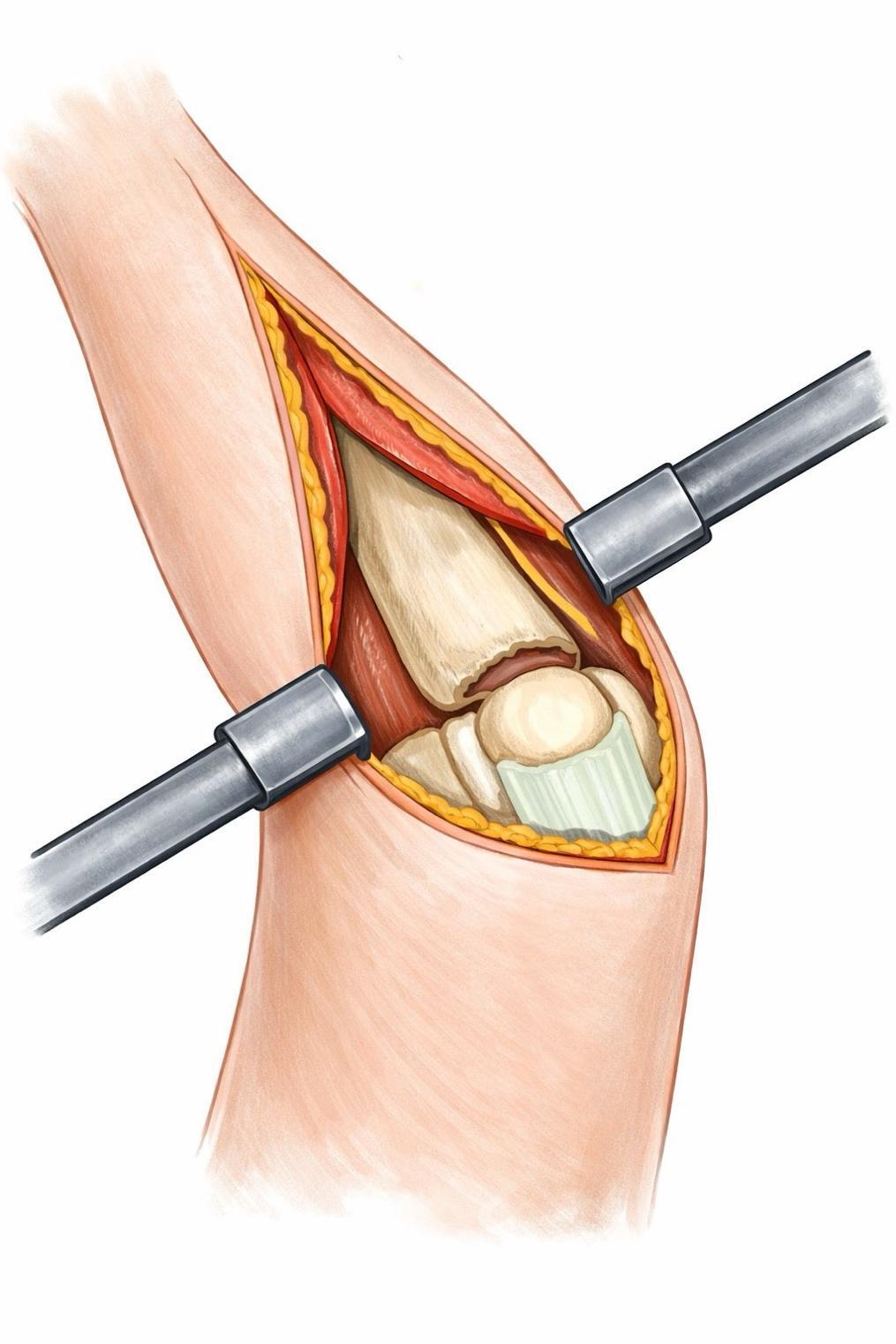
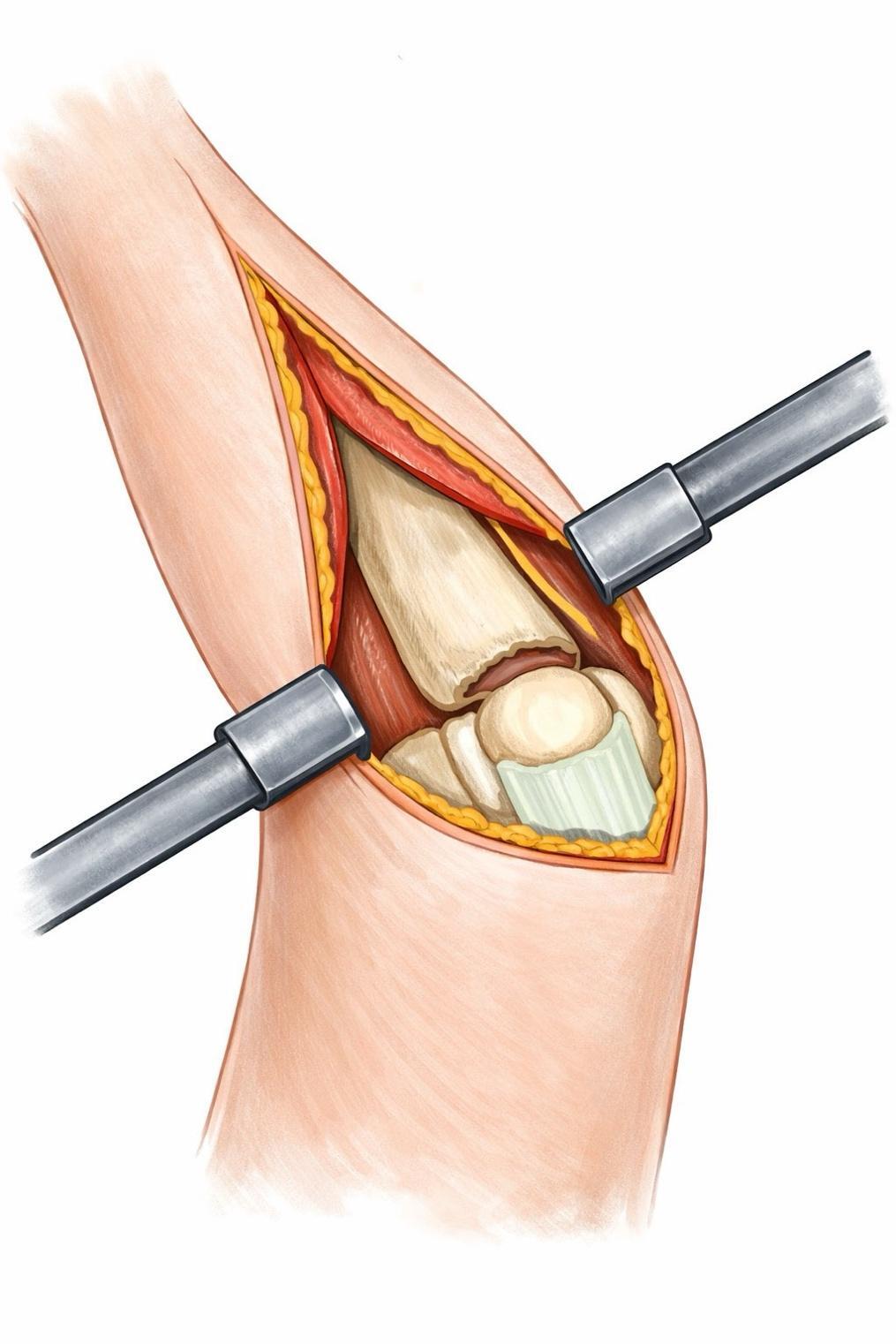
Twenty milliliters of 1% lidocaine with epinephrine are injected at the surgical site to provide postoperative analgesia and improve hemostasis. A posterior approach to the elbow is performed using an incision curved radially around the olecranon tip. Exposure is extended from the triceps tendon insertion proximally to about 8 cm distal to the olecranon tip. Full-thickness soft-tissue flaps are elevated down to the ulna periosteum. The ulnar nerve is identified but not routinely dissected. The fracture site is exposed, and the periosteum at the fracture margins is sharply elevated to allow clear visualization of the fracture edges to facilitate reduction. [Figure 3] After evacuation of the fracture hematoma or early fracture callus, the joint is inspected for articular impaction, cartilage wear, or loose bodies, which should be removed. We have found that mild articular impaction, which is common even in stable fracture patterns, does not preclude stable fixation using the MSTB technique. Impacted articular segments can be carefully pried up and elevated with a Freer elevator, with the option of packing allograft bone behind it for added stability.
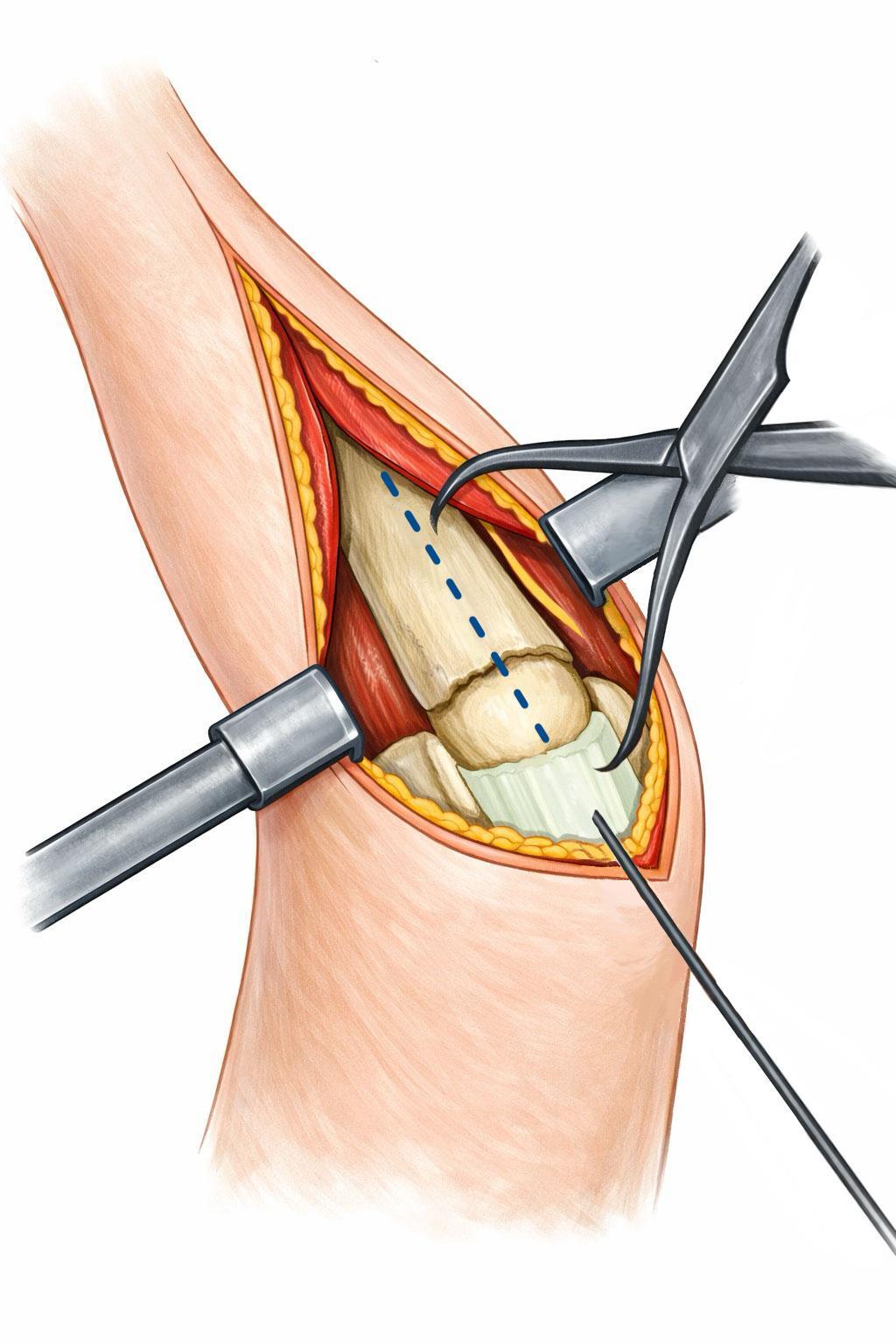
Fracture Reduction
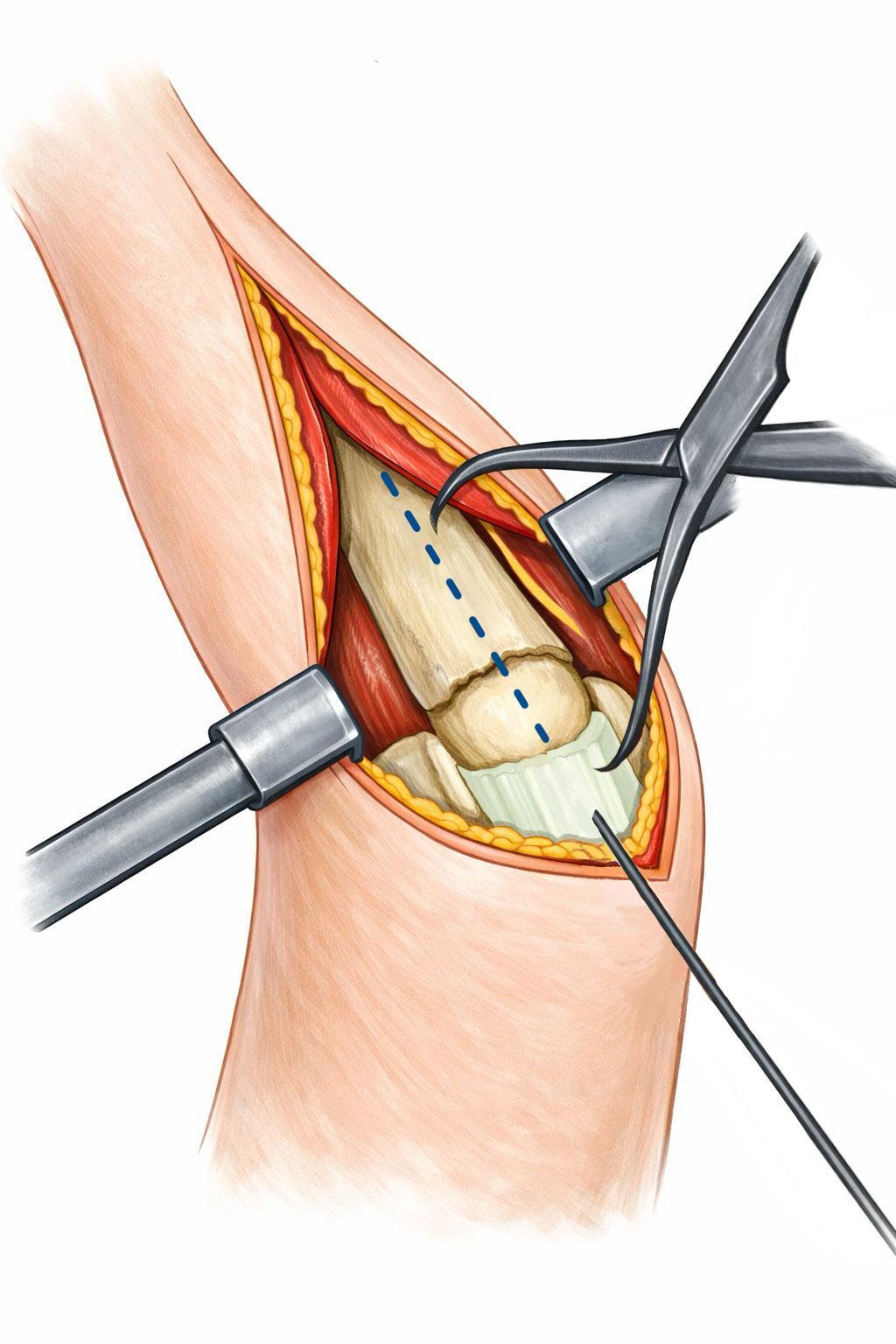
A towel clamp placed in the triceps tendon is used to manipulate the proximal olecranon fragment and achieve anatomic reduction to the ulnar shaft. The elbow is held in relative extension to relax the triceps to facilitate reduction. A pointed reduction clamp may be applied to maintain provisional alignment. [Figure 4] A guidewire for the HCS is then inserted in an antegrade, longitudinal direction through the triceps insertion and into the central part of the proximal fragment. The wire is advanced across the fracture site and into the central ulnar metaphysis, providing provisional fracture fixation. Supplemental oblique Kirschner wires may be placed, if desired, to further secure the fracture. We typically use a 4.0-mm HCS (Acutrak 3 Standard size), which requires a 0.054-inch guidewire.
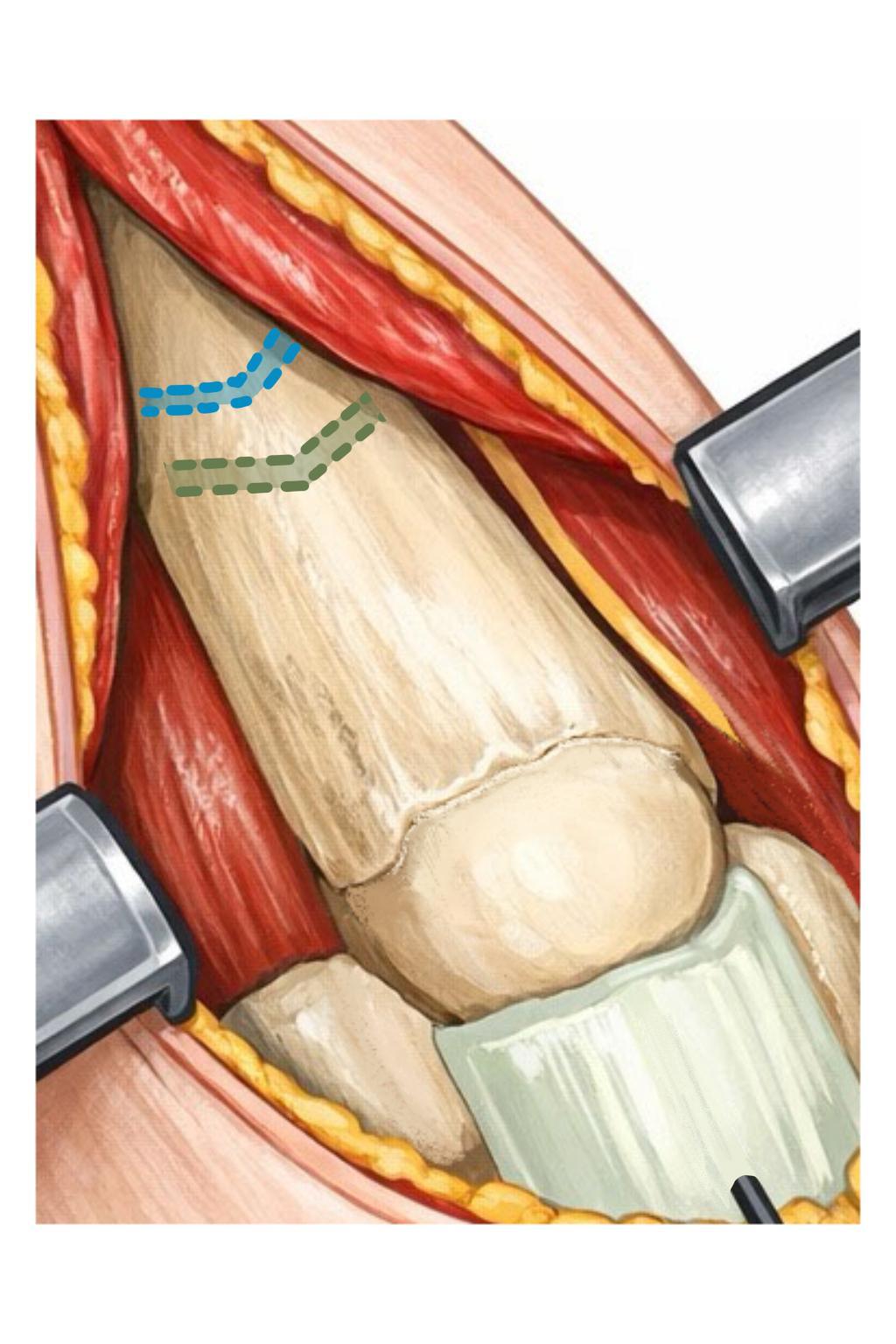
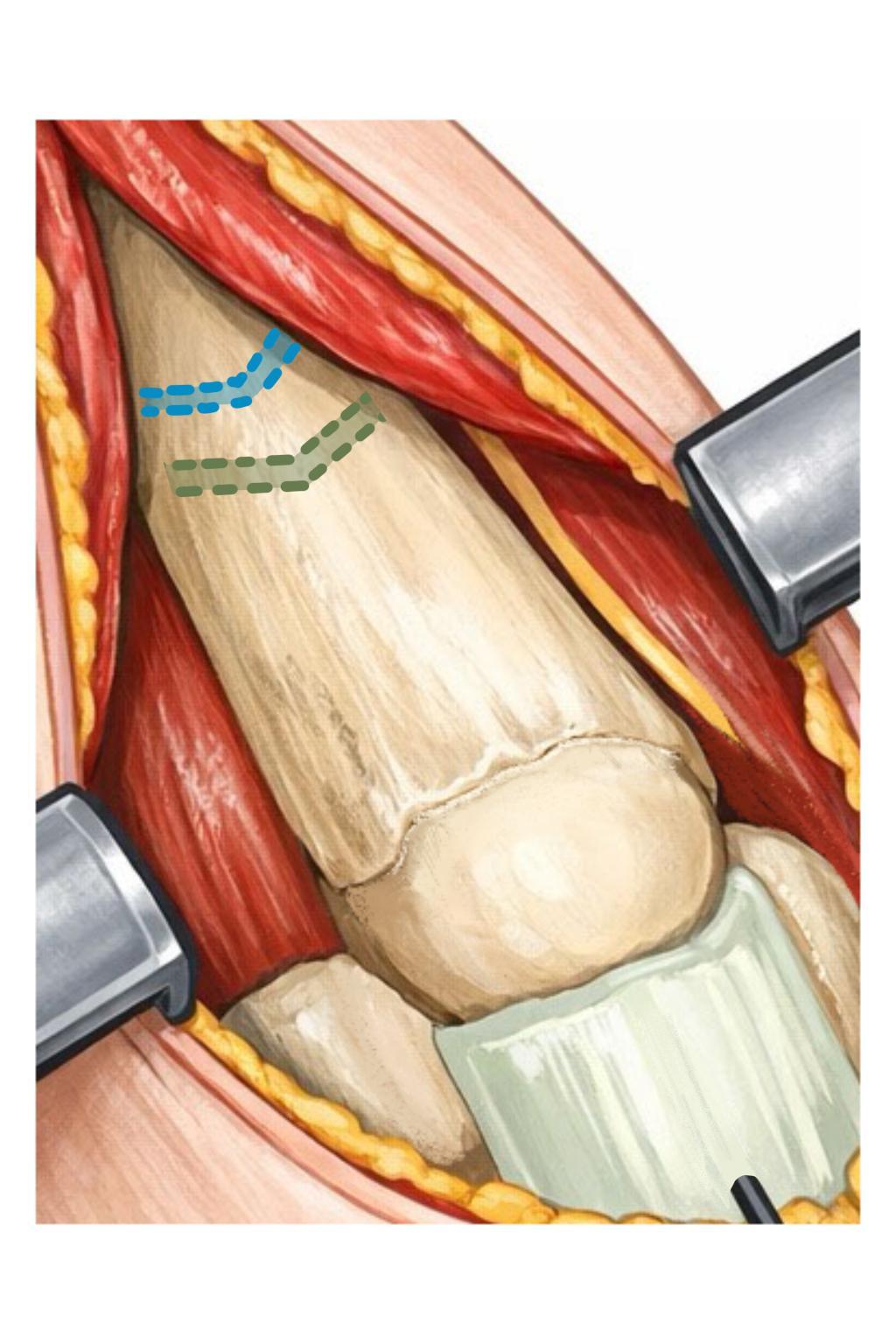
Bone Tunnels
Attention is then turned to the construction of the dual STB construct as described by Phadnis and Watts, with one modification: two ulna bone tunnels are created instead of one. The use of two tunnels simplifies suture passage (one suture tension band per tunnel) and provides redundancy should one bone tunnel fail. The ulnar periosteum and muscle insertion, including the anconeus, is elevated from approximately 3 to 6 cm distal to the fracture. Final suture knots will ultimately be buried beneath the anconeus muscle. Using a 2.5-mm drill bit, two transverse-oriented bone tunnels are created approximately 4 cm and 5 cm distal to the fracture line. [Figure 5] The tunnels are drilled in a V-shaped configuration, which facilitates needle passage and preserves a robust bone bridge. Care should be taken to ensure that the tunnels are within cortical (and not metaphyseal) bone, maintain at least 5 mm of bone bridge on the ulnar ridge, and remain distal to the anticipated position of the tip of the HCS.
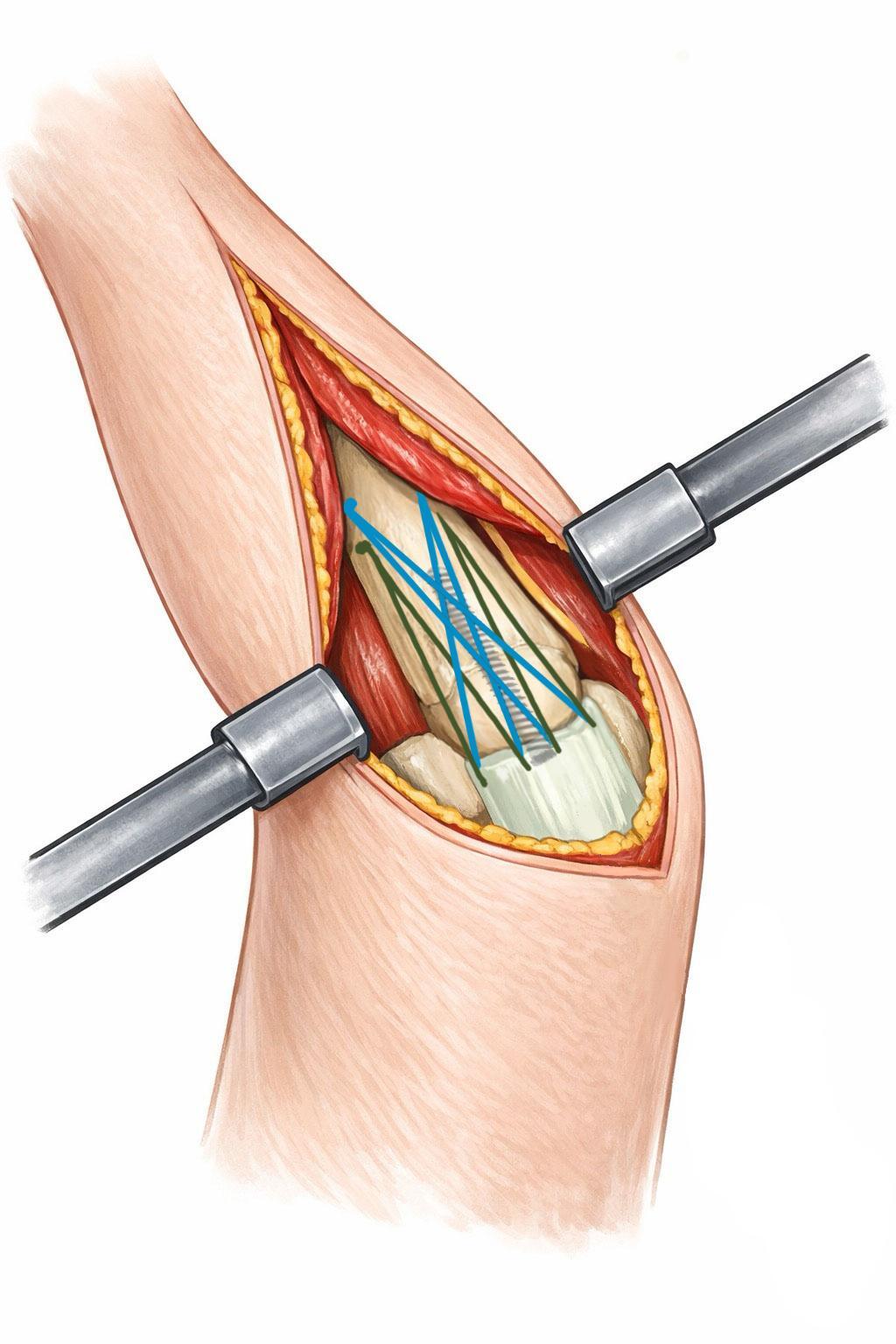
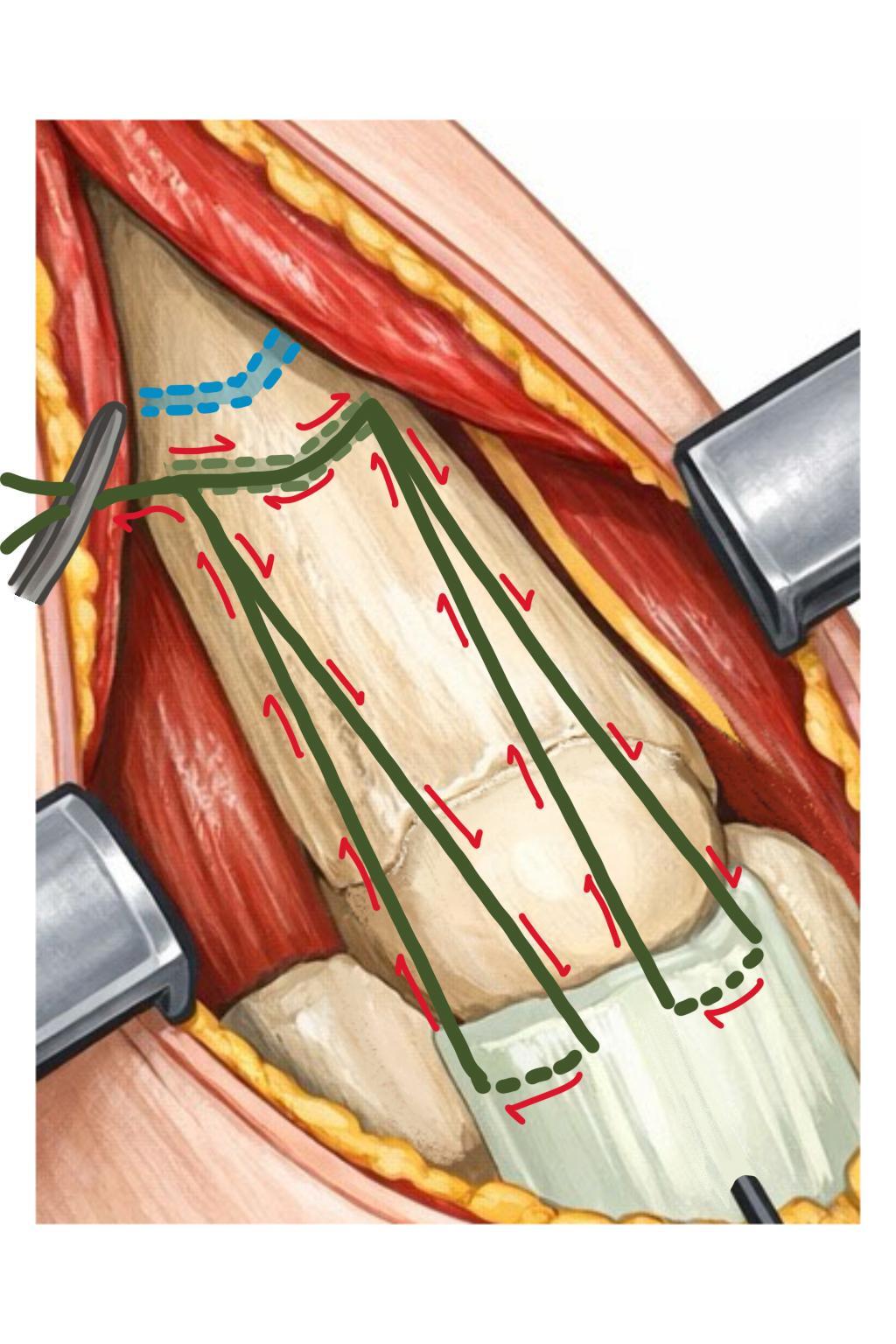
Suture Tension Bands
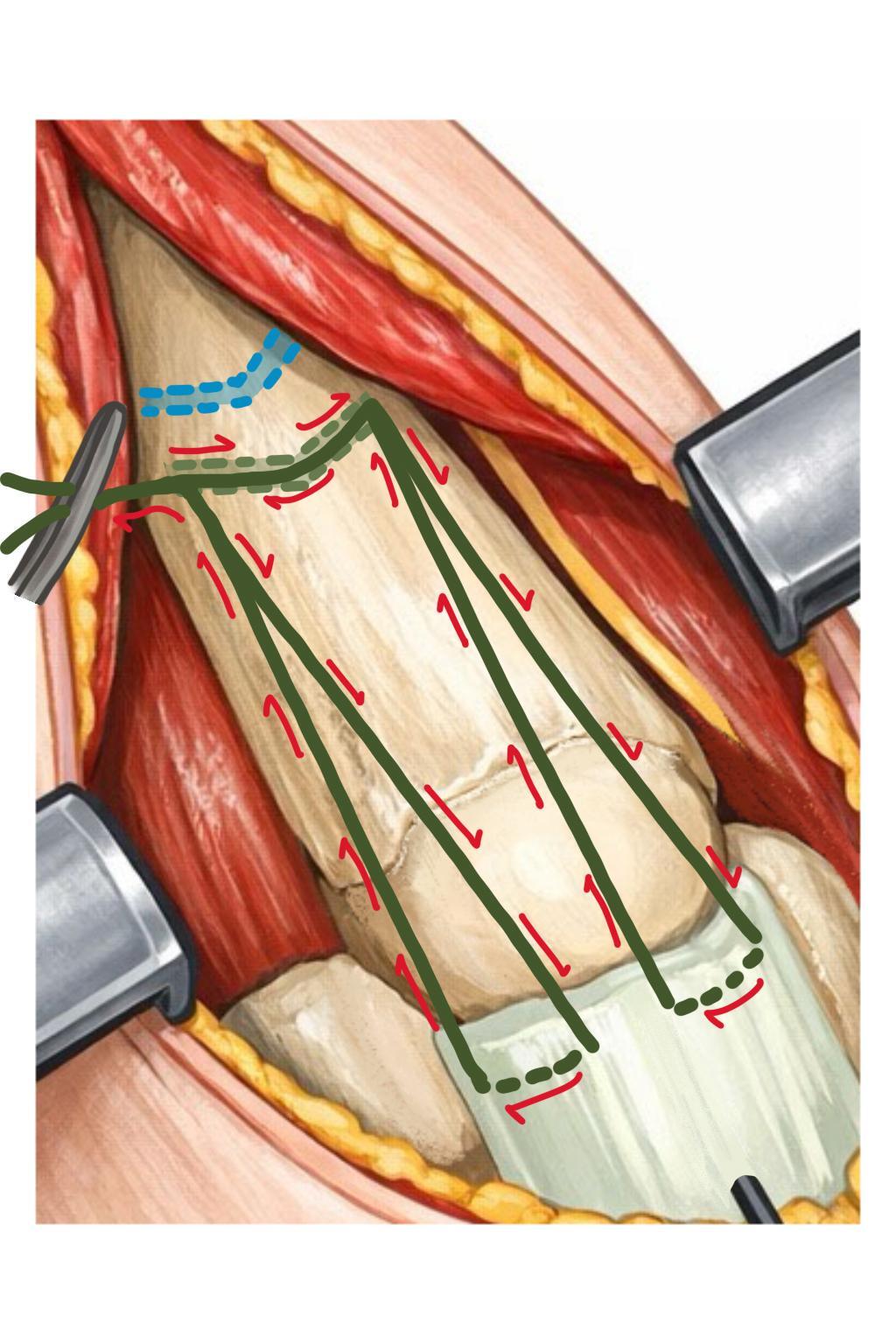
A #2 nonabsorbable, 2nd generation, high-strength braided suture (i.e., FiberWire, Arthrex, Naples, FL, USA; Orthocord, Depuy Synthes, Raynham, MA, USA) is used to create a box stitch through one of the bone tunnels and the triceps tendon. [Figure 6] The suture needle is first passed from radial to ulnar through the bone tunnel and then passed with a “generous bite” transversely through the ulnar half of the triceps tendon insertion. It is important that the needle hugs the bone to prevent the tendon from bunching during tensioning. Ideally, the needle should not cross the midline of the triceps tendon to avoid the anticipated path of the HCS. Though the HCS guidewire, if placed properly, should be slightly more anterior to the stitch path, in the central portion of the fracture fragment. The suture needle is then passed back through the same bone tunnel from ulnar to radial, taking care not to capture the previously placed suture limb. Finally, the suture is passed through the radial half of the triceps tendon insertion in a mirror fashion. The suture is then cinched firmly and secured with two provisional knots.
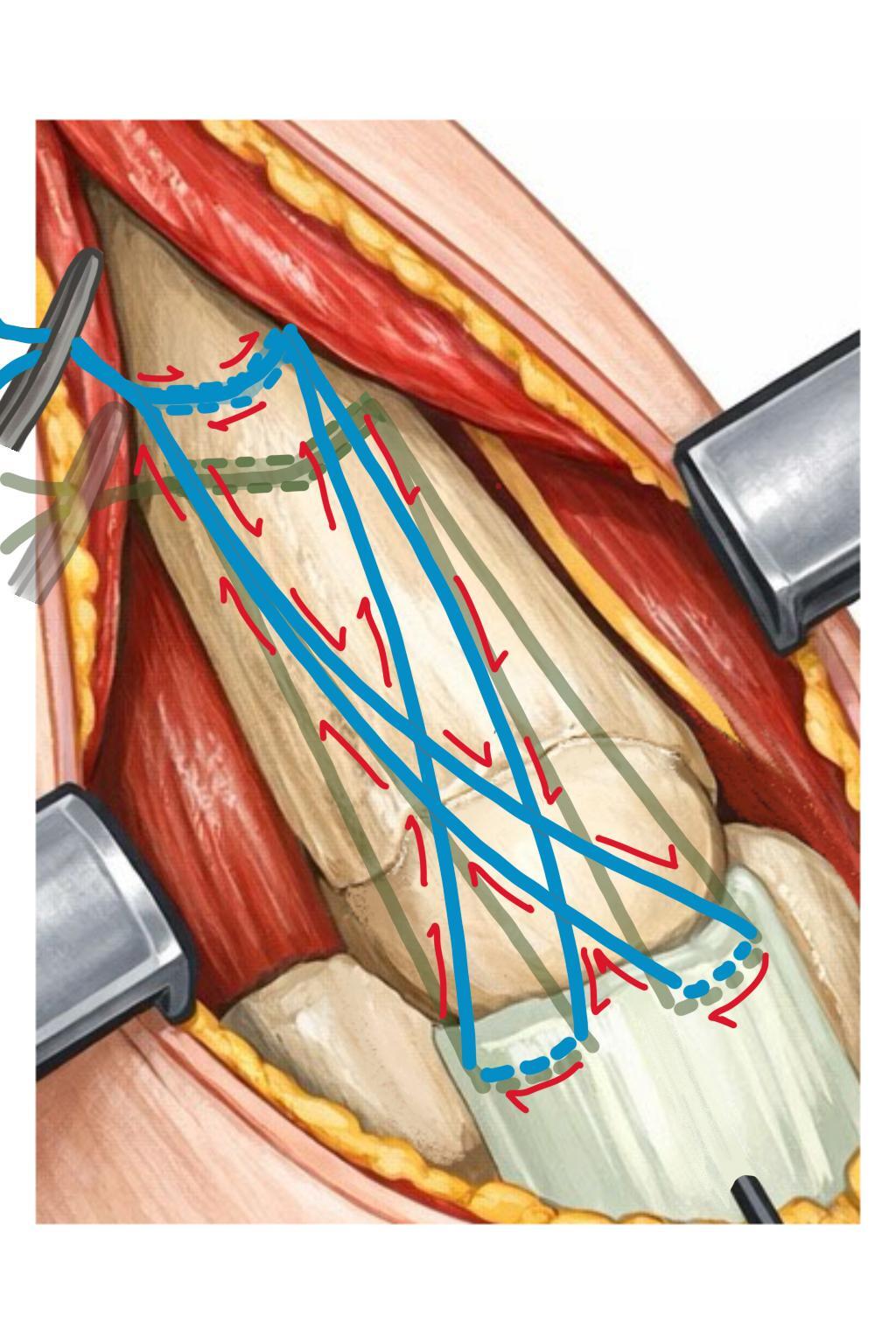
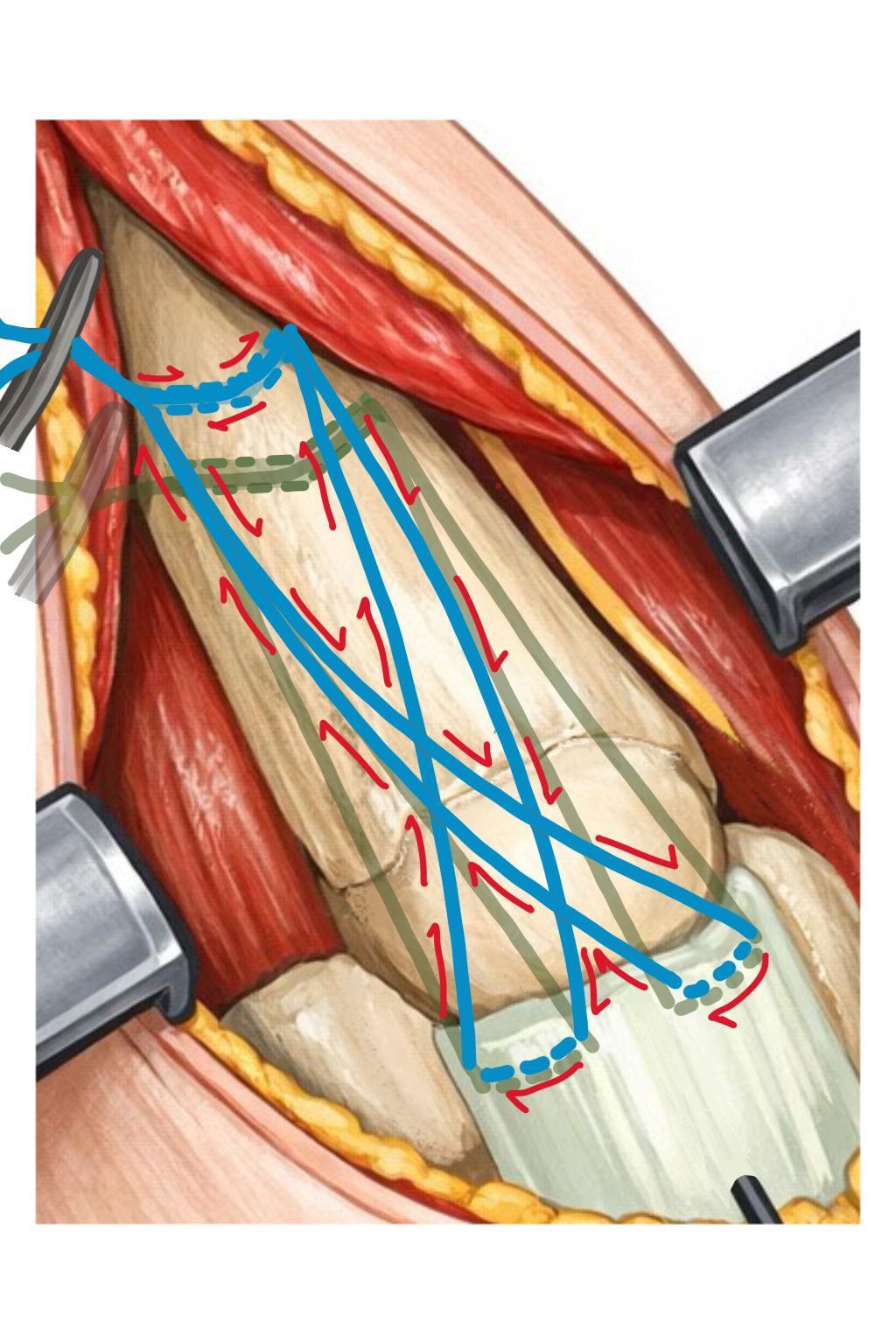
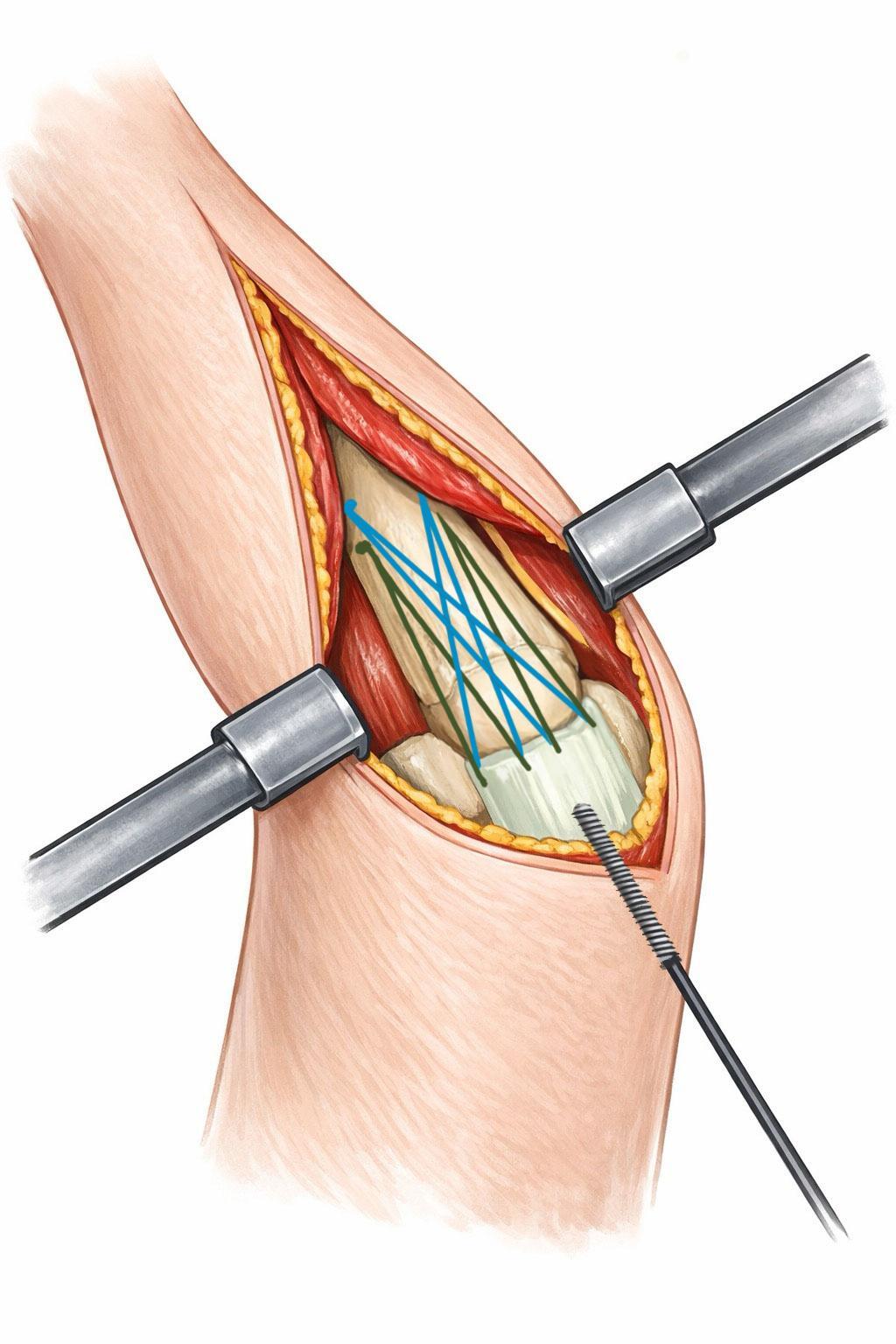
A second #2 nonabsorbable braided suture is used to create a crossing stitch through the second bone tunnel and the triceps tendon. [Figure 7] This suture needle is passed through the bone tunnel, again, from the radial to ulnar direction. The suture then crosses the midline of the ulna and is passed with a “generous bite” transversely through the radial half of the triceps insertion, ensuring that the needle remains adjacent to the bone. The suture needle is then passed back through the bone tunnel from ulnar to radial and subsequently passed through the ulnar half of the triceps insertion, creating a figure-of-eight configuration. The suture is tightened firmly and secured with two provisional knots.
Headless Compression Screw
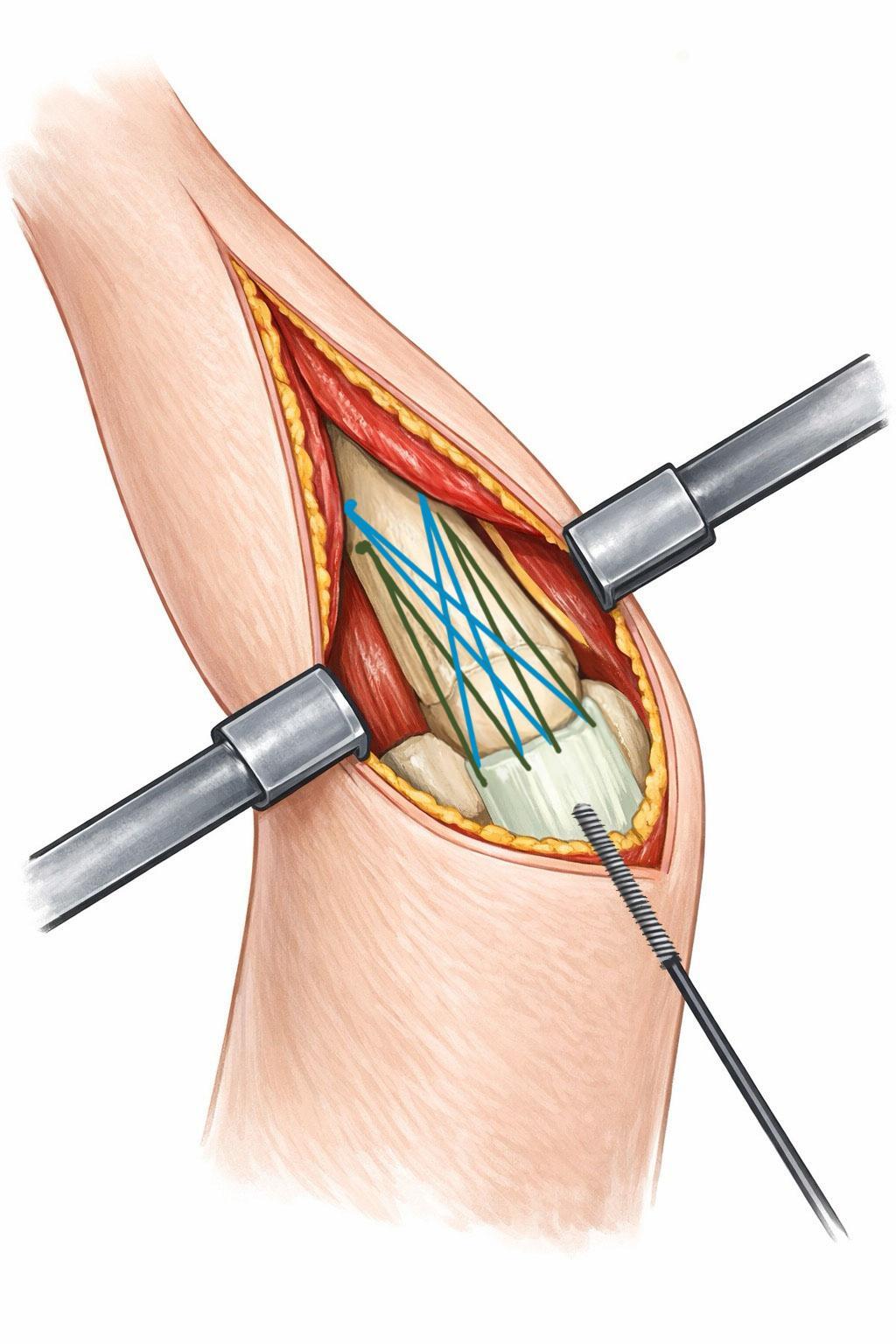
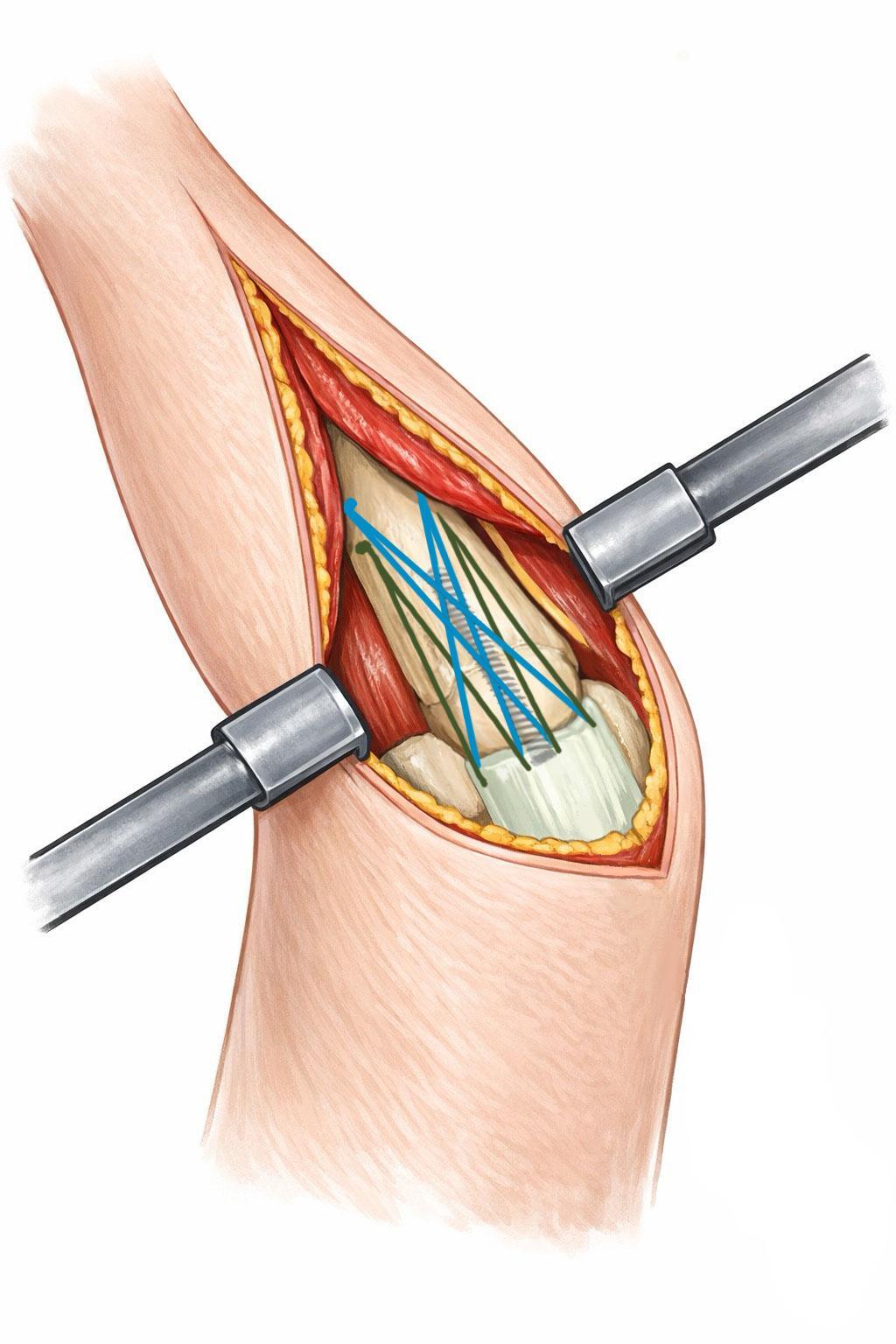
After confirming satisfactory fracture reduction both visually and fluoroscopically, a longitudinal stab incision is made over the guidewire, down to bone, and the HCS cannulated drill is advanced to the planned screw depth. [Figure 8]
Care should be taken not to advance the drill up to the bone tunnels, which could entangle and damage the tension band sutures. In our experience, a 4.0-mm diameter HCS provides adequate compression within the metaphyseal bone. A 34-mm screw length typically spans the fracture without encroaching on the bone tunnels, although screw diameter and length can be adjusted based on individual anatomy. The screw is inserted and tightened under lateral fluoroscopic guidance to ensure that the screw head is buried just below the cortex at the triceps insertion. Final fracture reduction is confirmed fluoroscopically. [Figure 9]
Re-tensioning and Construct Stability Check
The provisional suture knots are then sequentially released using two Adson pickups. Each suture is re-tensioned firmly to remove slack and secured with multiple knots placed, tied distally so that the knots can be placed beneath the anconeus muscle. This two-stage tensioning technique helps reduce suture creep and construct loosening. After insertion of the HCS, increased laxity in the tension band sutures is often observed, reflecting additional fracture compression and possible stress relaxation of the suture construct. After final knot tying, the elbow is taken through a full range of motion to confirm smooth motion and fracture stability without gapping in full flexion. Collateral ligament stability is also assessed.
Wound Closure
The procedure is typically performed with a tourniquet, which is released at this stage. Hemostasis is obtained using electrocautery. The tension band knots are positioned beneath the anconeus flap to bury them, and the investing fascia is closed over the top using a running 3-0 absorbable suture. Skin closure is performed according to the surgeon’s preference. Our preferred method is buried interrupted 4-0 Monocryl sutures, followed by a running 4-0 subcuticular barbed suture (Quill, Corza Medical, Westwood, MA, USA). The incision is sealed with skin adhesive, and longitudinal Steri-Strips are applied. A damp gauze is placed over the Steri-strips for approximately 20 seconds to facilitate rapid polymerization of the skin glue. A Mepilex dressing and ACE wrap (All cotton elastic wrap) is then applied. The arm is placed in a sling for comfort. Patients who require early weight-bearing or who are unlikely to comply with postoperative precautions may be immobilized in a posterior elbow splint at 90° of flexion.
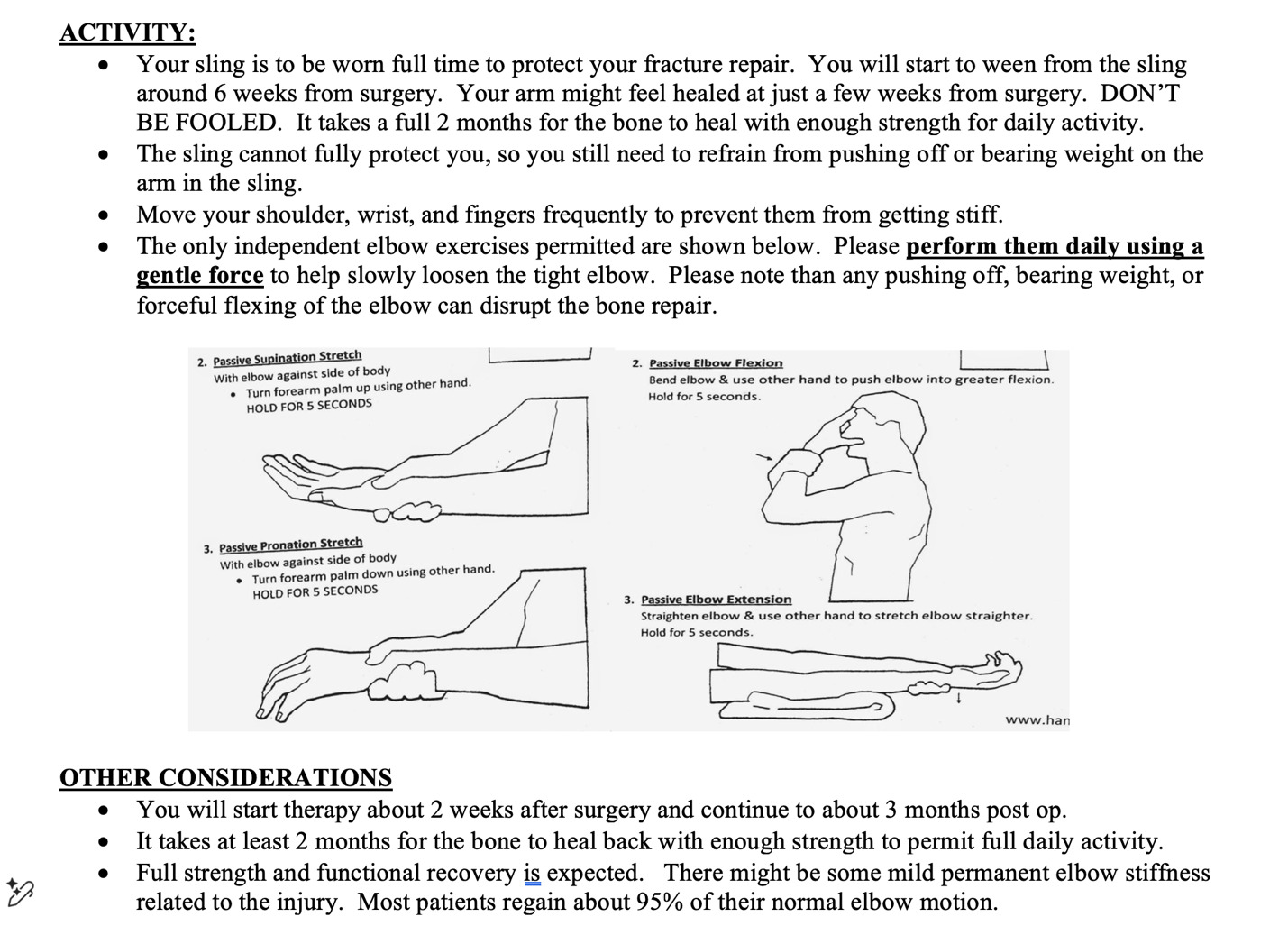
POST-OPERATIVE PROTOCOL
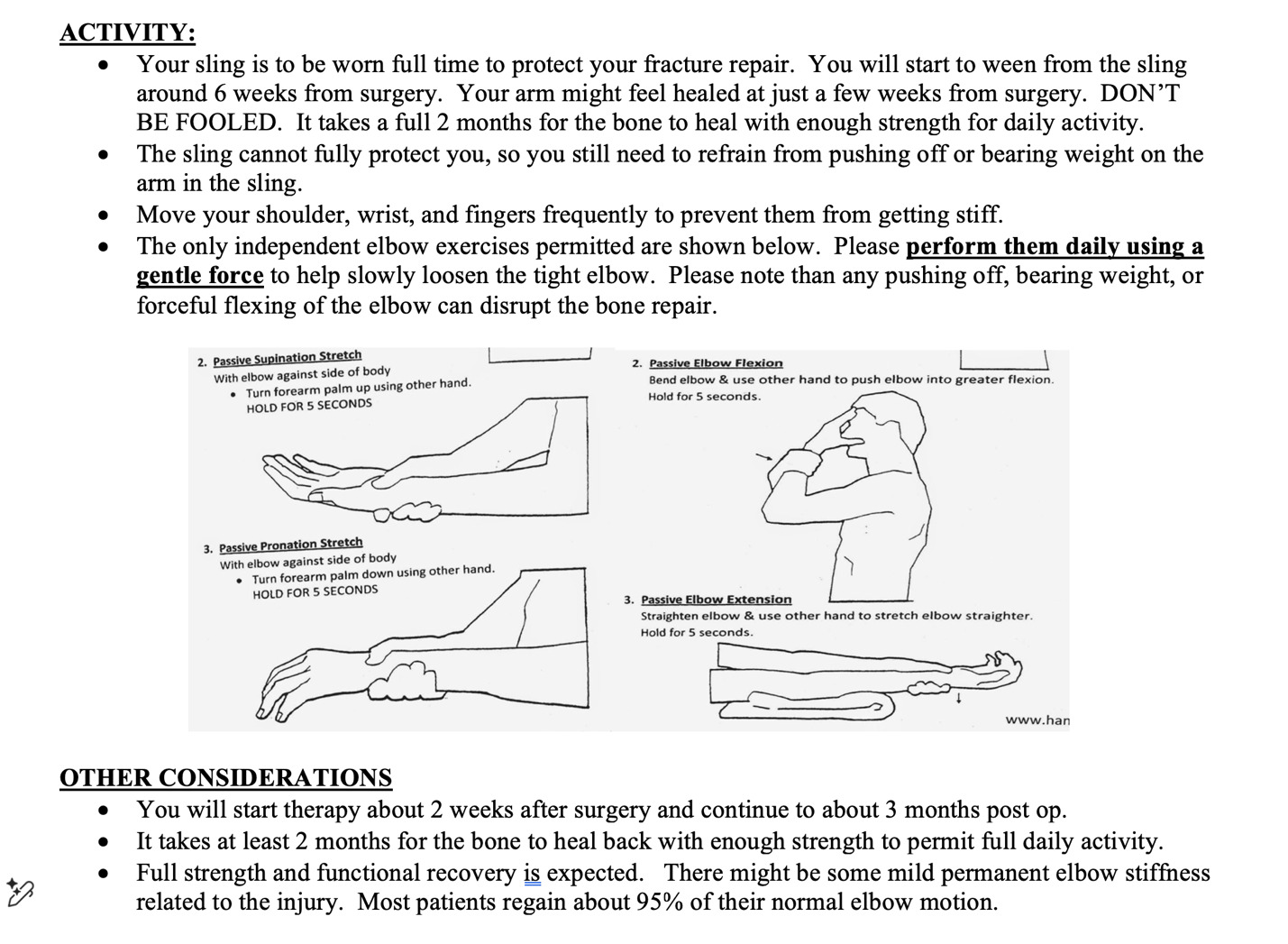
For compliant patients with stable fixation, a sling is worn full-time except during showering and prescribed home exercises. During showering, patients are instructed to keep the arm at their sides. Patients are instructed to remove the sling at least 4 times per day (with every meal) for approximately five minutes each to perform active and active-assisted elbow range-of-motion exercises, as illustrated in their postoperative instruction materials. [Figure 10] Shoulder, forearm, wrist, and finger motion exercises can be performed frequently while the arm remains in the sling.
Formal physical therapy is initiated at two weeks postoperatively. Patients begin weaning from the sling at four weeks, and strengthening exercises are initiated at six weeks, provided that fracture healing is progressing appropriately clinically and radiographically. Most patients are permitted to return to full unrestricted activity at approximately three months following surgery.
POTENTIAL COMPLICATIONS
As with all surgical procedures, superficial or deep hardware-associated infection is a potential complication. The lack of prominent subcutaneous hardware with the MSTB technique might reduce the risk of wound breakdown and infection compared to plating. Construct failure may occur due to bone tunnel fracture, suture laxity, or suture breakage, potentially resulting in fracture separation, delayed union, or nonunion.
Although symptomatic hardware is less common with this technique compared with traditional fixation methods, it remains a potential risk, particularly if the suture knots are not adequately buried beneath the anconeus muscle.
PEARLS AND PITFALLS
Bone tunnel orientation
Drill bone tunnels in a “V” trajectory on the ulnar shaft such that the needle on the tension band stitch passes freely. Different needle radii of curvature might require different drill hole trajectories. We have found that the #2 Fiberwire with a 26.5 mm tapered ½ circle needle has an ideal shape. If you are unable to pass the needle, the hole can be opened with a larger drill bit (i.e., 3.0mm) or a suture passer, and a free needle can be used.
Avoiding construct laxity
The suture tension band construct can loosen due to many potential causes, including suture stretch, bone tunnel widening, tendon bunching, and loose knots. It is important to reduce all sources of construct laxity to ensure a stable construct:
-
Place sutures through the triceps tendon as close to Sharpey’s fibers as possible, which will limit loosening from tendon deformation and bunching.
-
Perform provisional suture tensioning before placing the HCS, and re-tension afterward. This will address creep in the suture and system.
-
Tension the sutures with maximum force and use a snap to secure the surgeon’s knot before making the second throw.
-
If there is any gapping of the fracture with full elbow flexion, re-tension your suture tension bands
Headless screw placement
Appropriate placement and length of the HCS is important to avoid “wrapping up” or tearing the tension band sutures. First, be sure the screw guidewire is clear of the anticipated placement of the tension band stitches in the triceps tendon. Err on placing the guidewire and screw more anteriorly to avoid the triceps stitches. Secondly, the screw length should be chosen so as not to encroach on the suture in the bone tunnels. The screw does not need to be any longer than the metaphyseal segment and, in fact, will not get any purchase in the IM canal anyway. We have found that approximately 34 mm is the appropriate screw length.
DISCUSSION
We consider the MSTB to be an advantageous technique, as it largely eliminates the need for plate/screw constructs and wire tension band fixation, both of which are associated with hardware prominence and removal rates reported as high as 82%. The STB technique, in published studies and in our experience, has not required hardware (suture) removal, with only a single reported case of symptomatic suture knot sensitivity.⁷˒¹² It is applicable to Mayo type 2 fractures, which comprise approximately 90% of olecranon fractures, and is particularly well suited for cases with small proximal fragments or poor bone quality, both of which pose challenges for traditional fixation methods. Notably, neither STB nor MSTB fixation has been associated with proximal fragment escape, a complication reported with plate fixation in the setting of poor bone quality or small proximal fragments. In our experience, MSTB is also simpler, faster, and less costly than plate fixation, and even more cost-effective than K-wire tension band constructs when accounting for the frequent need for hardware removal.¹³ The learning curve is minimal, as the technique relies on bone tunnel and tension band principles familiar to most orthopedic surgeons.
We believe the addition of a headless compression screw (HCS) enhances construct stability by minimizing fracture separation. However, prior studies have demonstrated satisfactory outcomes with STB alone.²˒⁷ Isolated STB fixation may further reduce cost, operative time, and potentially eliminate the need for intraoperative fluoroscopy. These advantages make the technique particularly appealing in cost-conscious healthcare systems and resource-limited settings where implants and fluoroscopy may be less accessible. Additionally, as with many hand and elbow procedures, this technique can be performed using wide-awake local anesthesia without tourniquet (WALANT), further reducing cost, operative time, and the risks associated with general anesthesia.
Our decision to incorporate an HCS was informed by a retrospective review of our initial 11 patients treated with STB alone. In several cases, early postoperative radiographs demonstrated subtle fracture gapping compared to intraoperative fluoroscopy, suggesting either construct laxity over time or sensitivity to suture placement and tensioning. Although 9 of 11 fractures healed uneventfully, one resulted in delayed union and another in nonunion. We suspect that early fracture separation may have contributed to these outcomes. To address this limitation, we added an HCS to the construct. This modification adds minimal operative time, avoids hardware prominence, and incurs only modest additional cost. In a subsequent prospective assessment of 11 patients treated with MSTB, all maintained reduction and achieved union without delayed or nonunion.
The primary limitation of this technique is its unsuitability for unstable fracture patterns, including Mayo type 3 fractures with joint incongruity, fractures distal to the bare area, and distal oblique patterns. These injuries typically require the stability afforded by plate-and-screw constructs with multiple fixation points and fixed-angle support. Similarly, elbow fracture-dislocations are not appropriate for this technique. Relative contraindications include mild articular impaction (which may be amenable to elevation and bone grafting) and mild metaphyseal comminution. In select cases, we have extended the indications to include such fractures with good success. Lastly, when adopting this technique, particularly early in the learning curve, or when instability is suspected but not evident on radiographs, it is prudent to have plate-and-screw fixation available as a backup.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
The institution does not require ethical approval for the surgical technique paper.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.