INTRODUCTION
Olecranon fractures are a relatively common orthopedic injury that comprises approximately 10% of all upper extremity fractures.1 Due to their intra-articular nature and instability secondary to the deforming forces of the triceps at its insertion, these injuries generally warrant surgical fixation. Even in minimally displaced fractures, there is a high risk of progressive displacement and the need for prolonged immobilization, which can compromise its outcome with non-operative treatment.
Overall, olecranon fracture fixation has positive outcomes and a low nonunion rate, with Karlsson et al. reporting up to 96% good to excellent results at 15-25 years.2 However, a thorough understanding of the relevant anatomy and fixation strategies is necessary to avoid potential complications such as wound breakdown, loss of reduction, or loss of elbow mobility. The purpose of this article is to review the surgical technique for two methods of olecranon fracture fixation: tension band wiring and locking compression plate fixation.
INDICATIONS AND CONTRAINDICATIONS
Most olecranon fractures are indicated for operative fixation. Contraindications for operative fixation of olecranon fractures include active elbow infection, open fractures with gross contamination and loss of posterior skin, and/or generally compromised posterior soft tissue. Non or minimally displaced fractures, or fractures in patients unsafe for surgery, can be treated non-operatively. However, non-operative treatment may require prolonged immobilization with potentially secondary displacement or stiffness. There is also evidence that even displaced or comminuted fractures in elderly patients may be treated non-operatively, with an estimated 75% of cases developing a fibrous but functional nonunion.3
Tension band wiring constructs with Kirschner wire (“K wire”) fixation are best indicated for simple, isolated, displaced olecranon fractures without significant comminution, distal extension, or humeral-ulnar instability.4 This technique offers absolute theoretical stability by translating tensile triceps forces into compressive forces to facilitate early motion and primary healing across the fracture site.5 Locking plate fixation is best indicated for fractures with ulnohumeral instability, oblique or comminuted fractures, fractures involving the coracoid process, distal shaft extension, and trans-olecranon fracture dislocations.4,5
SURGICAL TECHNIQUE
Surgical Preparation
For either fixation technique of an olecranon fracture, the patient may be anesthetized with general anesthesia or sedated with a regional block. The patient may be positioned lateral or prone with the injured extremity being suspended with the hand down. Alternatively, the patient may be positioned supine with the injured extremity bent across the chest on top of pillows or blankets under the drape for support. A sterile tourniquet may be applied proximally at the upper arm. An incision is marked just lateral to the midline along the posterior elbow to avoid the skin directly overlying the olecranon tip. Prior to incision, a local anesthetic such as 10-20cc of 0.5% bupivacaine with epinephrine may be injected for postoperative pain relief. A miniature C-arm is used to capture intra-operative radiographs and confirm fracture reduction.
Surgical Equipment
For tension band wiring, necessary equipment includes: 1.6 or 1.5 mm K-wires, 1.2 or 1.0 mm stainless wiring, wire driver, drill with 2.0 bit, heavy needle drivers, wire cutter, tamp, mallet, and fluoroscopy.
For locking plate fixation, necessary equipment includes a 3.5 mm AO (Arbeitsgemeinschaft für Osteosynthesefragen) reconstruction plane or anatomically pre-contoured 2.5 to 3.5 mm locking olecranon plate and screws, drill, and fluoroscopy.
Tension Band Wiring
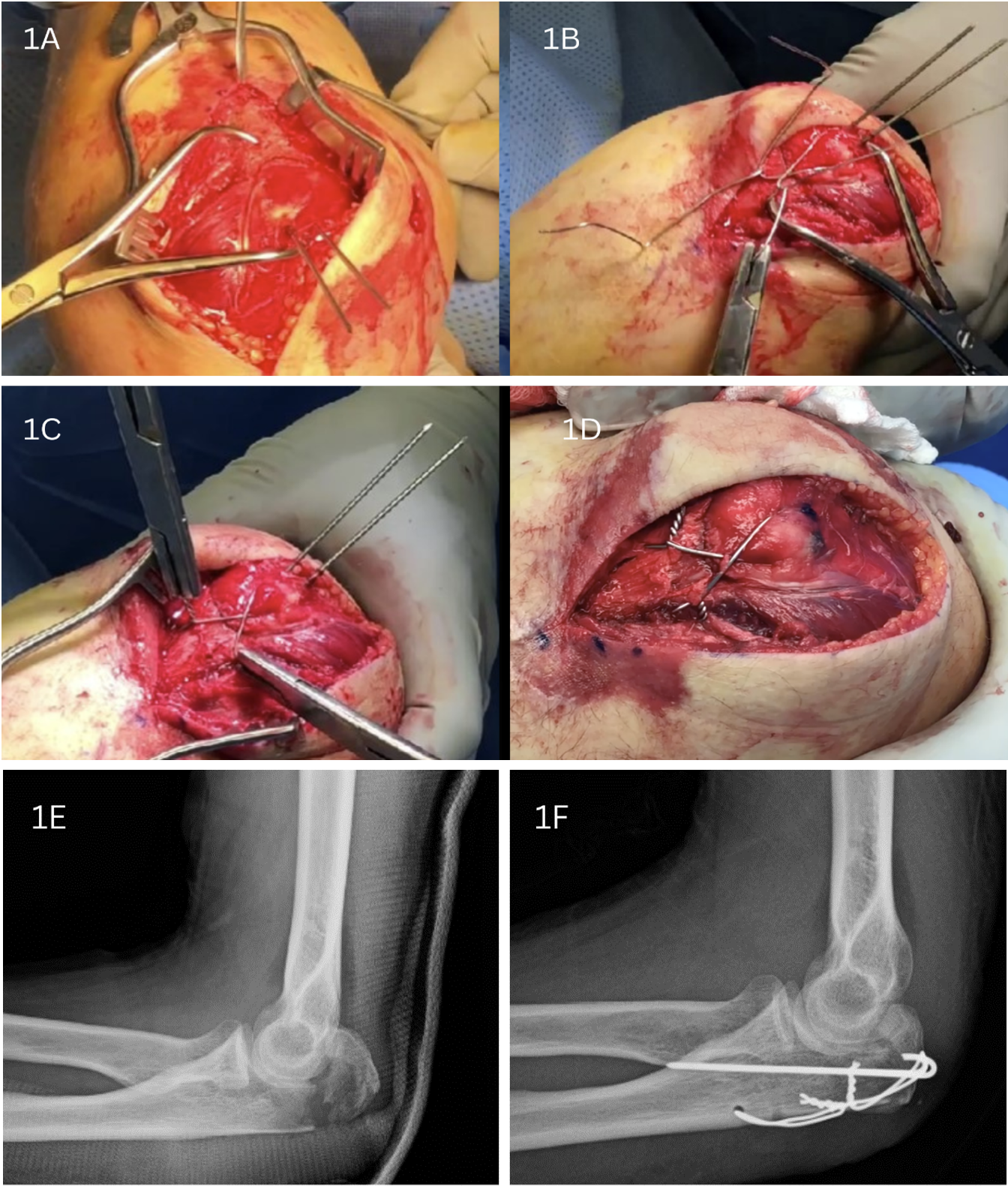
Following exposure with full-thickness skin flaps and debridement of the fracture site, a 2mm unicortical opening is drilled in the ulna, roughly 2-4 cm distal to the fracture site. A towel clip is placed across the proximal fracture fragment at the triceps insertion to help facilitate proximal ulnar fragment manipulation and fracture reduction. Pointed reduction forceps are placed across the fracture site, keying into the olecranon tip proximally and the unicortical pre-drilled hole distally. Utilization of these fixation points allows for sufficient space both proximally and distally for subsequent K-wire insertion. Surgeons should be cautious with reduction techniques in patients with osteoporosis or poor bone quality to prevent over-compression or further iatrogenic articular injury during reduction.
A 1.6 mm K-wire is then drilled antegrade through the posterior olecranon, roughly 20 degrees off the axis of the ulna, to accommodate the anatomic varus angulation of the ulnar shaft. A second 1.6 mm K-wire is inserted parallel and approximately 1-1.5 cm medial or lateral to the first K-wire. Subsequently, a transverse 2.5 mm bicortical drill hole is established roughly 3 cm distal to the fracture, anterior to the dorsal cortex. This is done from a medial to lateral orientation to protect the ulnar nerve. A 1.2 mm stainless steel wire is introduced through this pre-drilled hole in the ulnar shaft.
A second 1.2mm wire is then introduced proximal to the two inserted K wires across the dorsal ulnar cortex, deep to the triceps tendon, and across the proximal olecranon fracture fragment. The limbs of both the proximal and distal wires are connected on opposite sides across the fracture site. The wires are twisted around one another and tightened symmetrically with even tension. The excess wire is trimmed, and the tensioned knot construct is tamped down to the ulnar cortex on both sides to reduce soft tissue irritation and implant prominence. Attention can now be returned to the protruding 1.6 mm K wires in the posterior olecranon. To establish the hooked wire ends, the region where the wire penetrates soft tissue is marked using a sterile surgical marker. Each wire is then withdrawn 1 cm, grasped with a heavy needle driver at the marked site, and bent 180 degrees using the needle driver as a fulcrum. This wire is subsequently trimmed to a length of approximately 5 mm, rotated 180 degrees, and tamped into the posterior olecranon to capture the proximal end of the underlying tension band construct. Fluoroscopic confirmation of fracture construct and assessment of passive flexion, extension, pronation, and supination should be carried out at this time to ensure adequate fracture reduction and no prominent hardware between the anterior ulna and radius distally before the closure [Figure 1].

Locking Plate Fixation
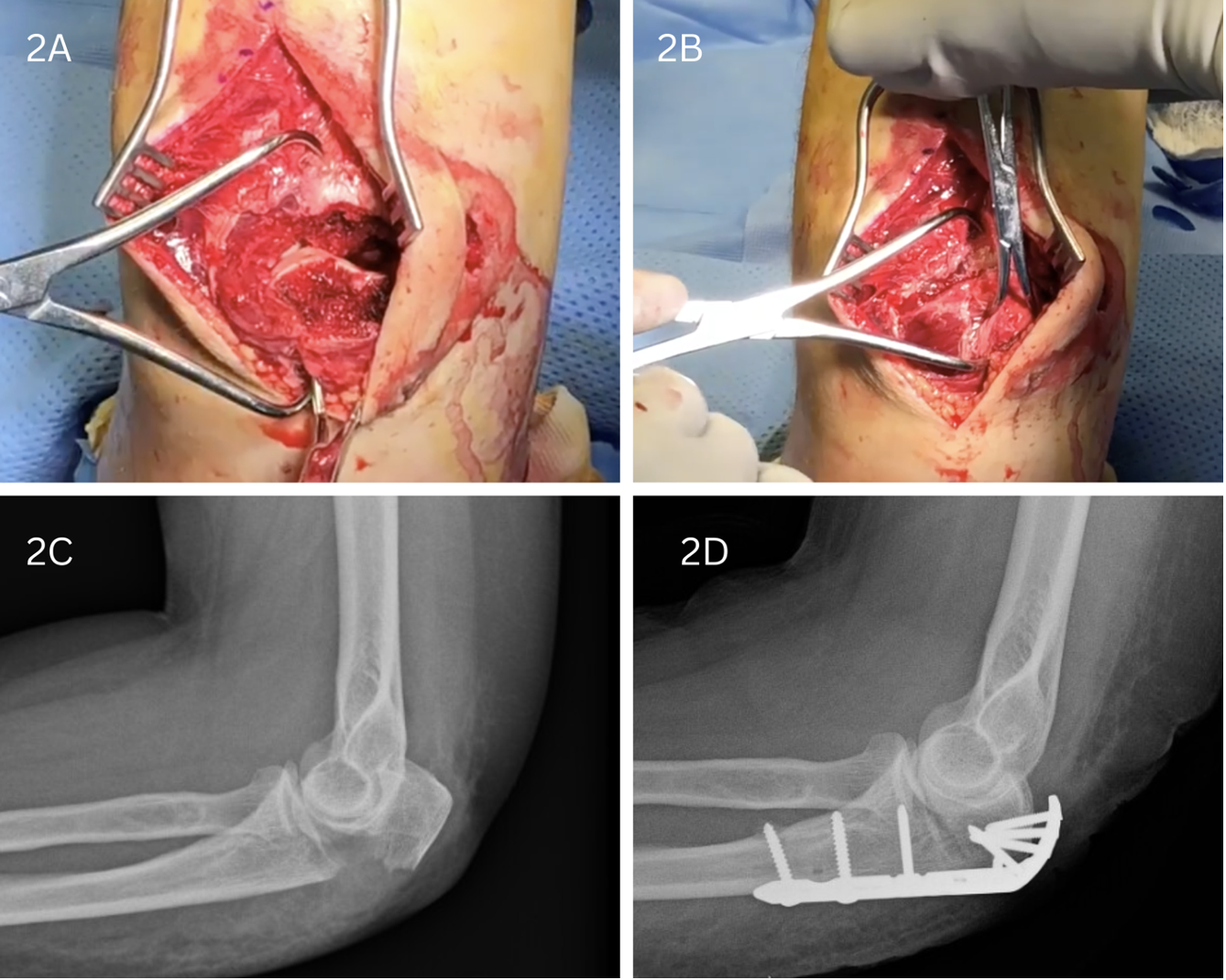
Once the fracture has been exposed and debrided, the reduction can be obtained using a point-to-point reduction clamp. Provisional 1.6 mm K-wires can also be drilled in the antegrade direction on either side of the reduced olecranon fragment to stabilize and hold the reduction. Either a 3.5 mm AO reconstruction plate is bent and contoured, or an anatomically pre-contoured locking olecranon plate is selected and applied along the dorsal cortex of the ulna. Once properly sized, the triceps is split longitudinally at the tip of the olecranon to allow for full seating of the plate on the dorsal posterior surface of the olecranon to fully capture the proximal fragment. Alternatively, the plate can be applied over the triceps tendon without splitting it. If possible, the plate can be pinned proximally and distally in place. Fixation is begun first distally by placing a cortical screw in the ulnar shaft in a compression fashion to secure the plate. Second, a non-locking compression screw is placed in the proximal aspect of the plate perpendicular to the fracture site and proximal to the bend of the plate for interfragmentary compression of the fracture as well as compression of the plate along the dorsal surface of the ulna. Before full compression, the distal shaft screw should be loosened to allow the plate to advance distally and re-tightened. Care should be taken that this posterior screw does not violate the articular surface of the trochlea of the ulnohumeral articulation. Once satisfied with the fracture reduction and plate positioning, the remaining holes are filled with unicortical locking screws proximally and bicortical non-locking screws distally.
Following confirmation of reduction and hardware positioning on fluoroscopy, the elbow is taken through a full range of motion to ensure the stability of the construct and no mechanical blocks to motion [Figure 2]. Of note, for any cases of intra-articular comminution, an arthrotomy from a medial or lateral approach can be performed to directly visualize the joint, facilitate reduction, or remove loose bodies. Furthermore, excessive dissection of the proximal olecranon fracture fragment should be avoided to preserve vascularity and compromise the triceps insertion.

Post-operative Management
The wound is thoroughly irrigated and closed in a layered fashion. The elbow is immobilized in a bulky soft dressing or a plaster posterior long arm splint for approximately 10-14 days which can be tailored based on the severity of the injury and surgeon preference. Patients are then subsequently instructed to resume the use of the arm for activities of daily living and initiate a passive and active-assisted range of motion exercises. However, strengthening and resistance training are withheld until fracture healing is confirmed between 8-12 weeks post-operatively to avoid the risk of fracture displacement. A complete list of pearls and pitfalls for surgical fixation of olecranon fractures can be found in Table 1.
DISCUSSION
Surgical treatment of olecranon fractures provides predictable, durable outcomes with high patient satisfaction rates. Karlsson et al. found 84% excellent and 12% good results in patients treated for olecranon fractures at a mean of 19 years postoperatively.2 Factors associated with worse outcomes include older age and increased injury severity; however, most patients still recover functional range of motion with low rates of persistent elbow pain.2,6 Additionally, nonunion occurs in as low as 1% of cases and is more frequent in high-energy injuries.7
While most patients regain adequate elbow function following fixation, complications can arise, which may impact the recovery process. Hardware irritation and removal is the most frequently encountered complication of olecranon surgery and has been reported to be as high as 82% in previous literature.8 However, hardware removal following fracture healing can typically be performed safely at an appropriate time interval without impacting fracture stability and often improves pain and satisfaction once addressed. Decreased range of motion following olecranon fractures is fairly common, which occurs most often with loss of terminal extension and is associated with symptomatic hardware or post-traumatic arthrosis.6 Although ulnar neuritis and infection are less common complications and a possible byproduct of the initial injury and postoperative inflammation, surgeons and patients should be aware of these risks throughout the perioperative period.
The preference of hardware for olecranon fixation may be controversial; however, no high-quality randomized studies demonstrate a superior method. Retrospective comparative studies have suggested some advantages and disadvantages to both techniques, but there have yet to be consistent differences in clinical outcomes. Hume et al. found a higher rate of loss of reduction and hardware discomfort in tension band constructs versus plate fixation.9 Others have found longer time to union and decreased range of motion in patients undergoing plate fixation compared to tension bands.10 Overall, we believe both constructs can provide stable fixation of olecranon fractures when performed by experienced surgeons. Our group prefers tension band fixation for simple, minimally-comminuted fractures that can tolerate compression at the fracture site. In contrast, plate fixation is reserved for more complex injuries with significant comminution and or fractures with distal shaft extension.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
The institutional review board at the Rothman Institute at Thomas Jefferson University does not require ethical approval for reporting surgical technique papers.
Declaration of informed consent
There is no information in the submitted manuscript that can be used to identify patients.
Acknowledgements
Not applicable