INTRODUCTION
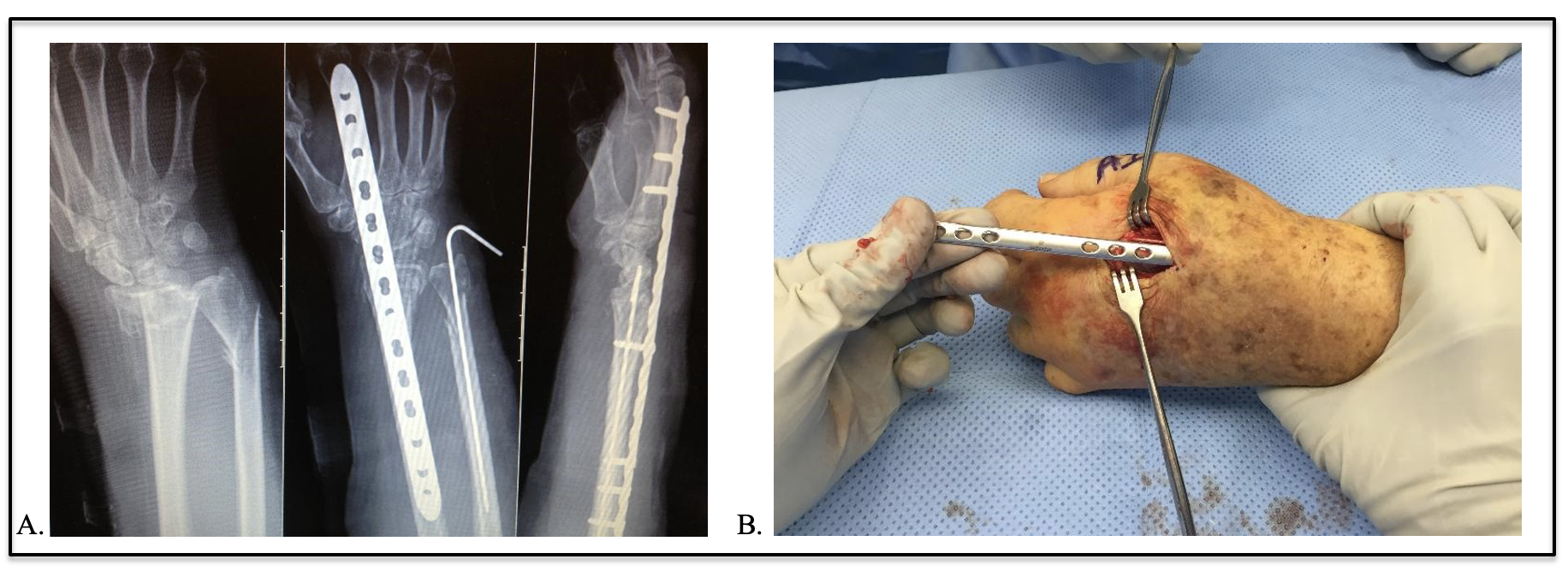
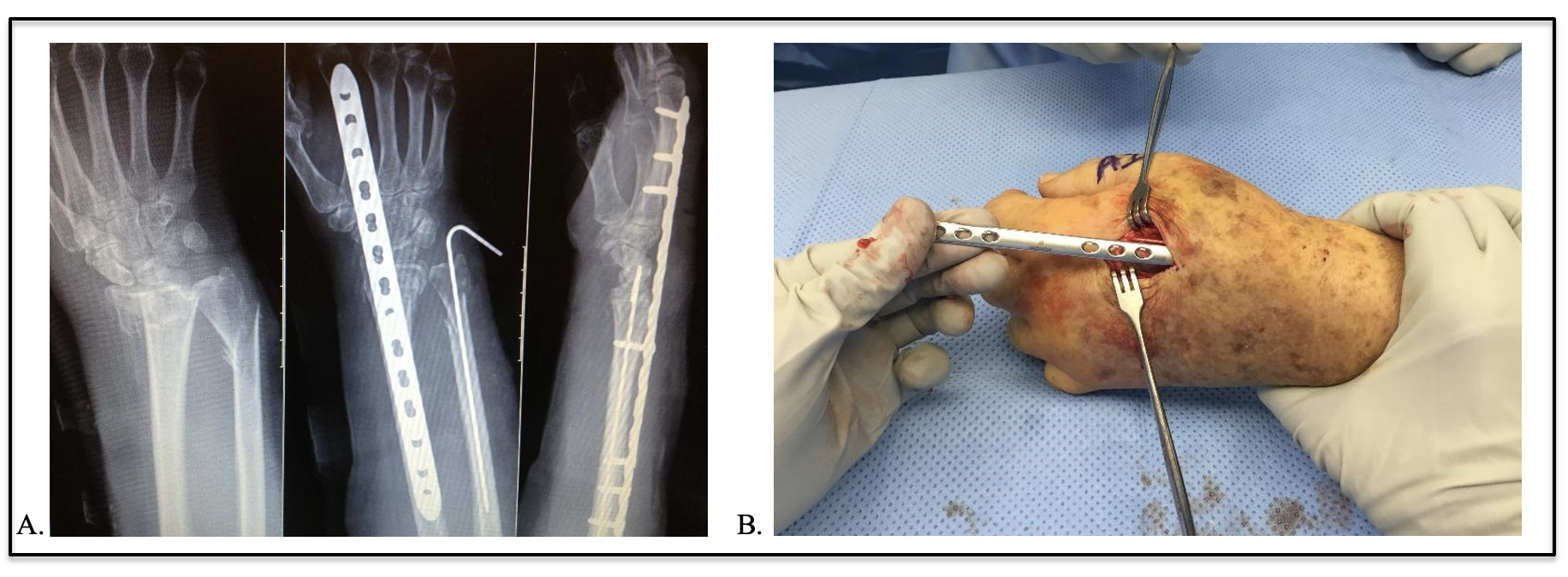
Distal radius fractures (DRFs) are among the most common fractures.1 While nonoperative treatment is common, surgical fixation is often indicated for patients who use their hands to ambulate, termed a functional quadruped, such as those who are walker-dependent or poly-traumatized, requiring crutches or other ambulatory assistive devices.2,3 Dorsal spanning bridge plate fixation has recently been popularized to manage fracture fixation in functional quadrupeds as it allows immediate weight-bearing across the injured wrist4,5 This technique initially utilized a dynamic compression plate; however, lower-profile anatomic locking plates have become more available [Figure 1].4
This report describes a case of an unexpected implant fracture of a low-profile anatomic spanning bridge plate from presumed fatigue failure due to repetitive load-bearing stress, resulting in EPL tendon rupture. A review of relevant literature, the plate’s failure analysis, and future recommendations for dorsal spanning bridge plate fixation are presented.
CASE REPORT
A 63-year-old, right-hand dominant female, previously an independent ambulator, presented following a fall from standing, incurring left hip and left distal radius fractures. After hip fracture repair, a dorsal spanning 2.4mm locking distal radius bridge plate (DePuy Synthes, West Chester, PA) was applied using the standard technique to allow for immediate weight-bearing with the injured wrist when using an ambulatory assistive device.
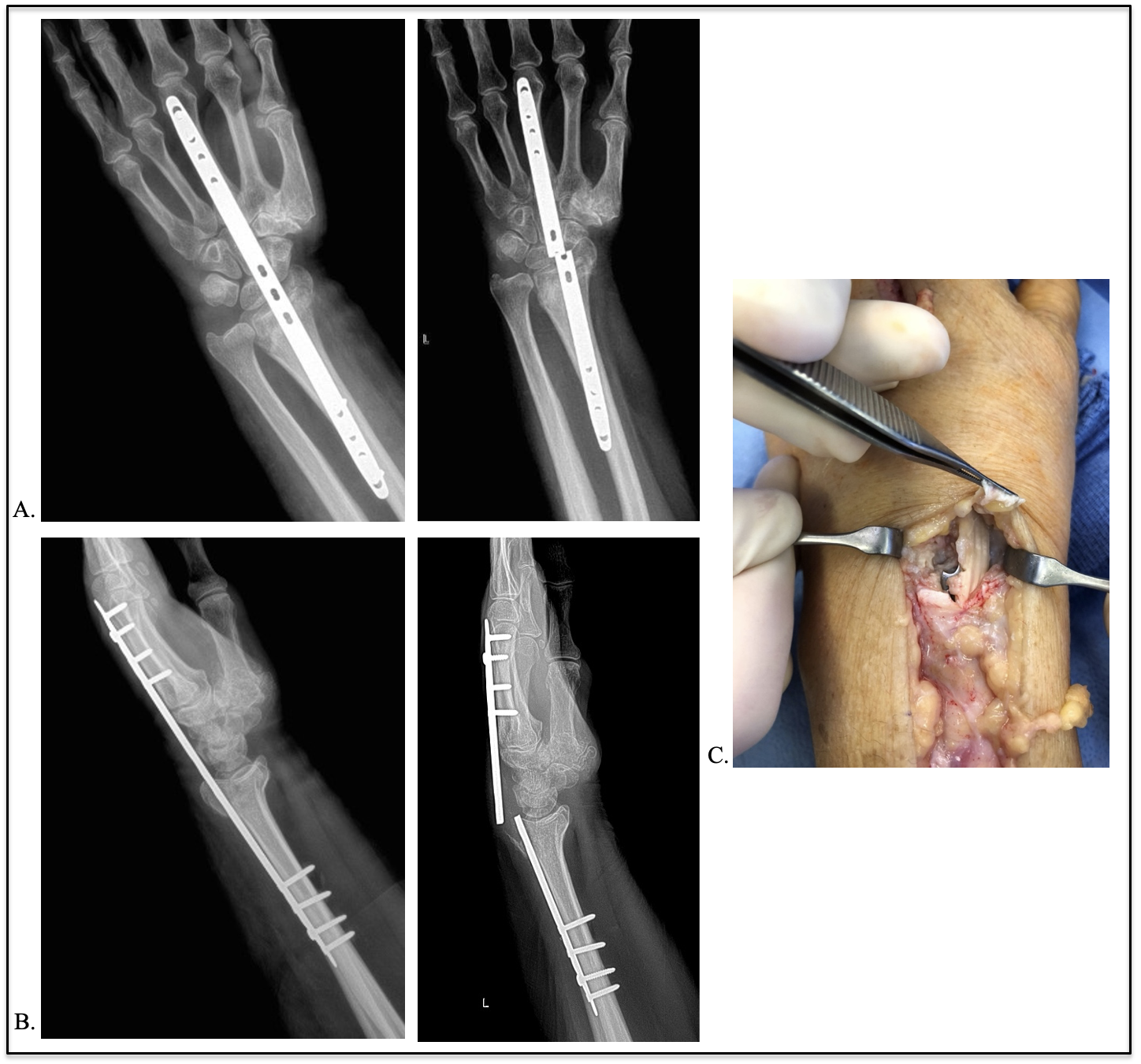
The surgery proceeded uneventfully. As intended, immediate weight-bearing through the repaired left wrist was allowed using a standard walker. Staged hardware removal was scheduled for 12 weeks postoperatively. However, at nine weeks postoperatively, the patient presented with acute onset wrist pain/swelling with increased motion and inability to extend her thumb. Of note, the patient previously had normal finger/thumb extension immediately post-operatively. Radiographs identified a fatigue fracture of the bridge plate through the central screw holes at the level of the wrist joint [Figure 2].
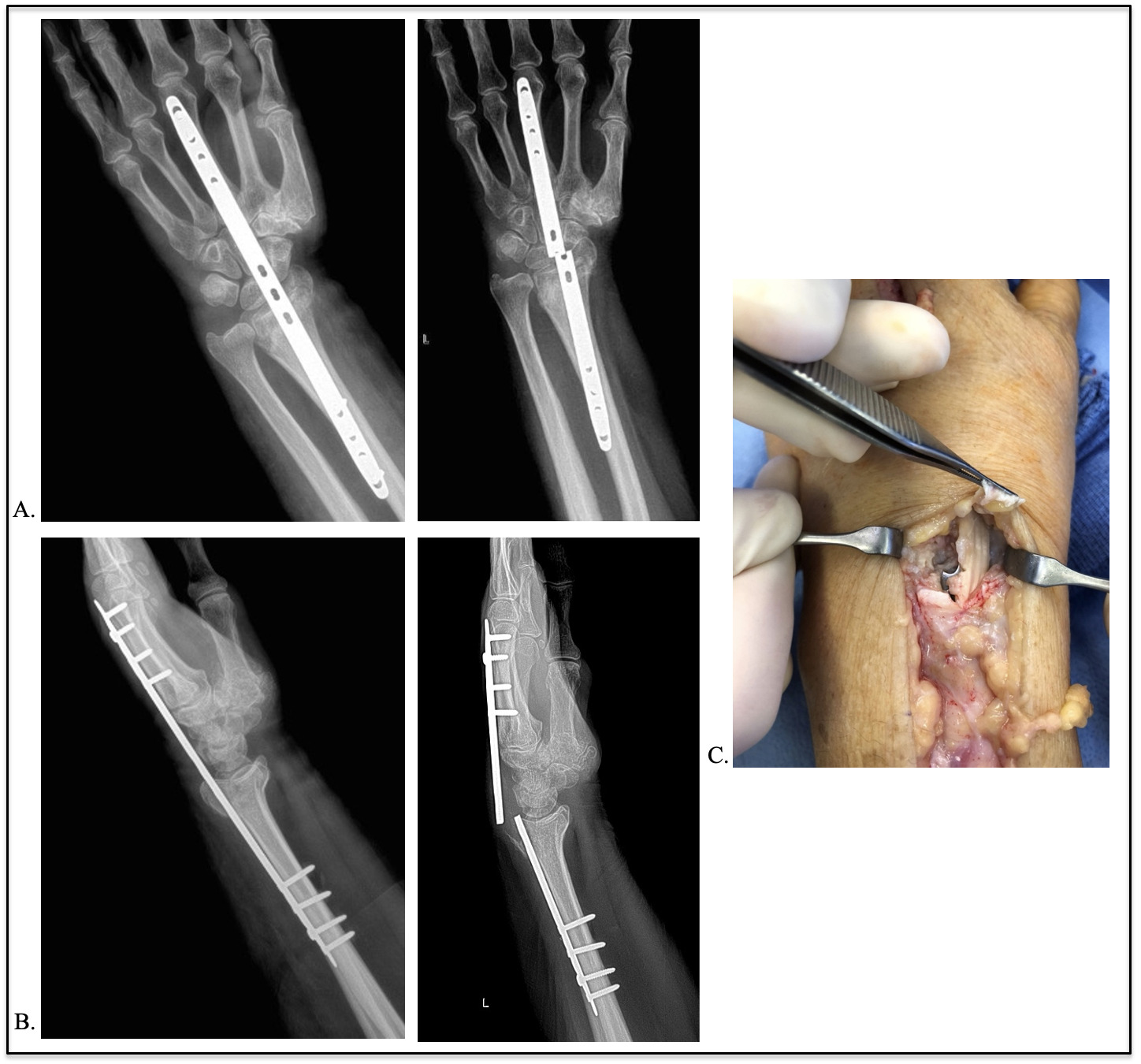
The patient received immediate surgical hardware removal and tendon repair. Satisfactory fracture healing was confirmed during this second surgery, with no additional internal fixation applied. Additionally, midsubstance rupture of the extensor pollicis longus tendon at the level of the plate’s fracture was confirmed and repaired with an extensor indicis proprius to EPL tendon transfer with no intraoperative complications [Figure 2]. Afterward, she was allowed to continue weight-bearing through the injured wrist and began tendon transfer rehabilitation immediately. The patient remained walker-dependent. No additional wrist intervention was required, with the last follow-up being approximately 13 months after the index surgery.
DISCUSSION
The dorsal spanning bridge plate construct has expanded from its original indications in managing highly comminuted distal radius fractures to include polytrauma patients with a goal of weight-bearing through the injured upper extremity.3,4,6 The original technique applied a 3.5mm dynamic compression plate in a non-compression and non-locked fashion.4 Recently, contoured low-profile locking plates have increased ease of application in functional quadrupeds with DRFs.5 This strategy of treating a functional quadruped during rehabilitation from a lower extremity injury resulted in fatigue failure of the bridge plate during allowed weight.
Burke and Singer first described dorsal bridge plating utilizing a 3.5mm dynamic compression plate with holes in the mid-section of the plate but did not report any fatigue failure of their constructs.4 Two similar studies looking at DRF treatment with 3.5mm dynamic compression plates in over 50 patients found one case of implant fatigue fracture.6,7 In this case, the radius fracture had healed, and uncomplicated hardware removal was performed.7
Hanel et al. reported on 62 patients treated for DRFs and requiring immediate upper extremity weight-bearing as functional quadrupeds, using 2.4mm locking dorsal spanning bridge plates with holes in the mid-section of the plate. One implant fracture was reported, having occurred at 16 months, with an associated extensor tendon rupture.8 A subsequent study focused on complications of over 140 patients treated with dorsal 2.4mm and 2.7mm locking bridge plates.9 Three cases of bridge plate fatigue fracture were reported, all at the level of the wrist joint through holes in the mid-section of the plate, prompting them to recommend using 3.5mm plates instead of 2.7mm to avoid future fatigue failure.
A cadaveric study by Huang et al. compared the axial load stability of dorsal spanning locking bridge plates to volar locking plates and concluded that the dorsal spanning locking bridge plates fatigued through mid-plate holes and therefore were inferior to volar plates.10 They thus advocated for improved plate design, notably the removal of midplate holes.
The location of distal plate fixation must be considered when minimizing the risk of bridge plate failure and tendon injury. Our patient’s plate was fixed to the third metacarpal. While there is evidence that distal fixation to the third metacarpal is biomechanically stronger,11 when compared to a distal fixation on the second metacarpal, one study found that plate fixation on the third metacarpal posed a greater risk of tendon entrapment and rupture.12 This increased risk of tendon rupture is likely due to the course of the plate along the intermediate column along the radius superficial to the EPL tendon.
This case report serves to caution that low-profile anatomic locking bridge plates with holes in the mid-section of the plate are at risk for early plate fatigue failure and tendon rupture with weight-bearing through the injured wrist. Plate designs with central screw holes at the wrist joint region are particularly at risk. Early fatigue failure of the plate can result in exposed or painful hardware and fracture displacement necessitating early surgery or additional unplanned surgical bone fracture fixation. Therefore, we recommend using either a 3.5mm locking dynamic compression plate or a low-profile 2.5 to 2.7mm anatomic locking bridge plate without mid-plate holes to avoid fatigue fractures when patients are expected to weight-bear through the injured wrist immediately following fixation.