Introduction
Osteoporosis is a common condition affecting about 19.6% of women and 4.4% of men over 50.1 The disease represents a significant source of morbidity with associated fragility fractures, most commonly of the spine, hip, and wrist. Hip fractures are among the most impactful sequelae of osteoporosis, with a one-year mortality rate of up to 30% and significant associated disability.2 With 260,000-300,000 hip fractures in the United States annually, and most of these injuries are associated with osteoporosis, effective osteoporosis treatment as a preventative measure is imperative.3
Given the high prevalence and morbidity of osteoporosis, orthopedic surgeons should maintain awareness of the disease and be well-versed in management. This review aims to outline the factors that drive osteoporosis, summarize diagnostic methods, and review medical and nonmedical management of osteoporosis.
Review
Pathophysiology/Etiology of Osteoporosis
Osteoporosis stems from multifactorial changes promoting greater bone resorption than bone formation. This ultimately yields decreased bone mineral density (BMD), subsequently increasing fracture risk with low-energy falls. One significant driving factor of osteoporosis is the withdrawal of estrogen that occurs during menopause.4 Estrogen inhibits osteoclasts, which are primary cells responsible for resorbing bone. The decrease in estrogen levels during menopause increases the lifespan and number of osteoclasts acting to resorb bone.4 This estrogen withdrawal stimulates T cells to stimulate osteoclasts and generate inflammatory cytokines and reactive oxygen species, leading to osteocyte and osteoblast apoptosis.5,6 Lifestyle factors also play an important role in osteoporosis development. Suboptimal weight bearing from disuse and a sedentary lifestyle can result in bone loss.7 In contrast, overuse can result in micro damage that causes osteocyte apoptosis and signals osteoclasts to resorb damaged bone.5 Other nonheritable risk factors like smoking, nutrition, medical comorbidities, and fall risk can predispose patients to osteoporosis and subsequent fracture.5 In addition to these known risk factors, 60-80% of peak bone mass at the end of growth is believed to be genetically determined,8 suggesting that even modification of the above risk factors may not completely prevent the development of osteoporosis in the aging population.
Diagnosis of Osteoporosis
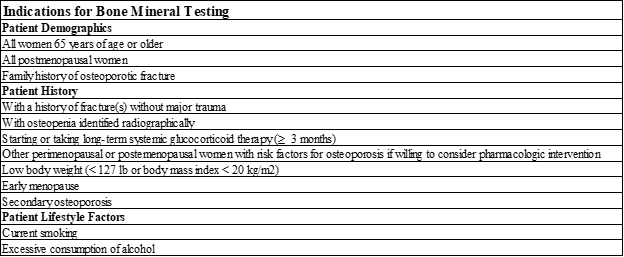
Diagnosis of osteoporosis is based on BMD, clinical history, and risk factors. BMD is evaluated with Dual-energy x-ray absorptiometry (DEXA) for patients fitting the criteria listed in [Table 1].9 Patients with a T-score of -2.5 or lower on DEXA scan of lumbar spine, femoral neck, hip, or distal 1/3 of the radius are diagnosed with osteoporosis.9 Patients with a T-score between -1.0 and -2.5 are diagnosed with osteopenia, and those with an increased fracture risk as determined by the fracture risk assessment tool (FRAX) are diagnosed with osteoporosis.9 Patients who have suffered a fragility fracture without other metabolic bone disorders, regardless of their BMD, are diagnosed with osteoporosis.9

Medical Management of Osteoporosis
Medical management is indicated for patients with osteopenia or osteoporosis.9 The first step in management is to measure 25-hydroxyvitamin D (25[OH]D) level and supplement with 1,000 or 2,000 International Units of Vitamin D3 to maintain a serum level ≥ 30 ng/mL along with 1,200 mg/day of Calcium.9 A recent meta-analysis by Liu et al. demonstrated that combined supplementation with Vitamin D and Calcium significantly increased total BMD, lumbar spine BMD, arm BMD, and femoral neck BMD and significantly reduced the incidence of hip fracture.10
Current drugs for osteoporosis can be categorized based on whether they are anti-resorptive such as bisphosphonates, selective estrogen receptor modulators (SERMs), denosumab, and calcitonin or anabolic such as parathyroid hormone (PTH) analogs, and sclerostin inhibitors. The first line of pharmacologic therapy for osteoporosis is generally bisphosphonates such as alendronate or ibandronate. Bisphosphonates can be given orally or intravenously and function by binding to bone minerals and are taken up by osteoclasts during resorption. This subsequently induces osteoclast dysfunction and apoptosis, leading to an anti-resorptive effect.11 Bisphosphonates effectively minimize osteoporosis-related fragility fractures, with a recent meta-analysis of 10 randomized controlled trials (RCT) of 23,284 patients showing that 12.4 months of therapy is needed to avoid one nonvertebral fracture.12 Bisphosphonates are contraindicated in patients with renal disease who have an eGFR < 30-35mL/min. Common side effects of oral bisphosphonates include upper gasterointestinal symptoms, reported in 20-30% of patients. Intravenous bisphosphonates can trigger a flu-like illness in 30% of patients after receiving their first injection. Rare complications of bisphosphonates are osteonecrosis of the jaw (incidence 0.2-10 per 10,000 patient-years) and atypical or “bisphosphonate-related” femur fractures (incidence 0.2 – 13 per 10,000 patient-years).11
SERMs such as bazedoxifene are another anti-resorptive therapy that interacts with estrogen receptors to have agonist or antagonistic effects based on the target tissue. At bone, they act as estrogen agonists and interact with the RANK-ligand/RANK/osteoprotegerin (OPG) system to decrease resorption.13 SERM efficacy for the treatment of osteoporosis and related injuries have been called into question as a recent meta-analysis of 107 trials, including 193,987 postmenopausal women, showed no significant reduction in relative risk of hip fracture for bazedoxifene (Relative Risk (RR): 0.92, 95% Confidence Interval (CI): 0.37-2.33) and raloxifene (RR 0.91, 95% CI 0.71-1.17). The study also showed no significant reduction in RR of nonvertebral fracture for bazedoxifene (RR 0.90, 95% CI 0.72-1.11) and raloxifene (RR 0.94, 95% CI 0.85-1.05). However, a significant risk reduction was shown for vertebral fractures for bazedoxifene (RR 0.61, 95% CI 0.41-0.90) and raloxifene (RR 0.59, 95% CI 0.46-0.76).14 The greatest safety concern for SERM use is thromboembolism and a 2008 meta-analysis of 9 trials including 24,523 patients demonstrated raloxifene use increases the risk of any venous thromboembolism (Odds Ratio (OR) 1.62, 95% CI 1.25-2.09), Deep Vein Thrombosis (DVT) (OR 1.54, 95% CI 1.13-2.11), and Pulmonary Embolism (PE) (OR1.91, 95% CI 1.05-3.47).15
Denosumab is an anti-resorptive, fully human monoclonal antibody that binds and inhibits RANKL, preventing the differentiation of osteoclast precursors to mature osteoclasts and inhibiting bone resorption.11 It has been shown to significantly reduce the risk of hip fracture (RR 0.56, 95% CI 0.35-0.90), nonvertebral fractures (RR 0.80, 95% I 0.67-0.96), and vertebral fractures (RR 0.32, 95% CI 0.22-0.45).14 Risks of denosumab use include skin rashes and infection; however, severe infection from immune dysfunction has not been observed.16
Calcitonin is a daily nasal spray that binds to calcitonin receptors on osteoclast precursors, preventing them from maturing and downregulating their function.13 A recent meta-analysis showed that calcitonin use could significantly reduce the risk for vertebral fractures (RR 0.65, 95% CI 0.50-0.85), while no significant risk reduction for hip fractures (RR 0.48, 95% CI 0.21-1.10) or nonvertebral fractures (RR 0.84, 95% CI 0.68-1.05) was observed.14 The most common side effects of calcitonin are rhinitis, nasal irritation, epistaxis, and allergic reactions.17 Additionally, a meta-analysis of 21 RCTs demonstrated an increased risk of cancer in patients using calcitonin (4.1%) compared with the placebo group (2.9%).18
PTH analogs, including teriparatide and abaloparatide, are anabolic therapies administered as daily subcutaneous injections. They act as PTH type 1 receptor agonists. The intermittent stimulation of this receptor leads to activation of the Wnt pathway, resulting in net anabolic effects on bone and upregulating transcription of OPG, which binds RANKL and causes an anti-resorptive effect.11 They are moderately effective, with a recent meta-analysis showing significant risk reduction for nonvertebral fractures for Abaloparatide (RR 0.51, 95% CI 0.29-0.87) and Teriparatide (RR 0.62, 95% CI 0.47-0.80) as well as significant risk reduction for vertebral fractures for Abaloparatide (RR 0.14, 95% CI 0.05-0.42) and Teriparatide (RR 0.27, 95% CI 0.19-0.38). The study showed a nonsignificant risk reduction for hip fractures for Abaloparatide (RR 0.24, 95% CI 0.01-4.84) and Teriparatide (RR 0.64, 95% CI 0.25-1.68).14 The most common side effects of PTH analogs include nausea, headaches, and transient hypercalcemia, more common in teriparatide (6.4%) than Abaloparatide (3.4%).19 Original studies in rats raised concern for increased risk of osteosarcoma; however, no association between teriparatide use and osteosarcoma has been found in humans with seven years of follow-up.20
Romosozumab is a humanized monoclonal anti-sclerostin antibody that serves as an anabolic agent. Sclerostin functions by inhibiting the Wnt pathway. Therefore, sclerostin inhibition with romosozumab activates Wnt, causing an anabolic effect to stimulate bone formation and inhibit bone resorption.11 A recent meta-analysis demonstrated that romosozumab use led to a significant decrease in incidence of vertebral fractures at 12 months (Odds Ratio 0.51, 95% CI 0.40-0.65) and 24 months (OR 0.43, 95% CI 0.35-0.52), nonvertebral fractures at 24 months (OR 0.708, 95% CI 0.66-0.92), and clinical fractures at 24 months (OR 0.70, 95% CI 0.60-0.82).21 A separate meta-analysis also found a reduced risk of vertebral fracture (RR 0.37, 95% CI 0.18–0.77), nonvertebral fracture (RR 0.79, 95% CI 0.68–0.92), and hip fracture (RR 0.59, 95% CI 0.42–0.83) at 24 months.22 Common side effects of romosozumab include injection-site reactions such as pain. Other adverse reactions include the risk of dermatitis, osteonecrosis of the jaw, and possibly cardiovascular events.23
Non-Medical Management
Lifestyle interventions can be implemented to preserve BMD and decrease fracture risk, especially in patients who may decline or not be appropriate candidates for pharmacologic therapy. Optimizing nutrition, particularly calcium and vitamin D intake, can benefit osteoporosis patients. Supplementation with calcium and vitamin D has been shown to decrease fragility fracture risk.24 A calcium-rich diet may be preferred over supplementation as it does not appear to carry the cardiovascular risk that calcium supplementation does while providing a comparable increase in BMD.25 Additionally, protein supplementation has shown inconsistent results regarding fracture risk, although current recommendations suggest adequate protein intake to maintain musculoskeletal function and decrease complications related to fractures.26 In addition to diet modification and supplementation, weight-bearing exercise in conjunction with other forms of exercise, such as strength training, has been shown to preserve BMD in postmenopausal women.27 A recent meta-analysis demonstrated that multicomponent exercise is associated with a 22% lower risk of falls and a 16% lower risk of fractures.28 Smoking cessation is also important as smoking is associated with an increased risk of fracture and lower BMD.29 Moderate alcohol intake has not been shown to be harmful to bone health, and it may be beneficial.22 However, greater than 2-3 drinks/day may damage bone health and is associated with increased fall risk.22
Conclusion
Osteoporosis is a common condition stemming from hormonal, lifestyle, and genetic factors resulting in weakened bones and increased fracture risk. Diagnosis is based on the presence of fragility fracture, DEXA scan, and fracture risk. Treatment involves adequate calcium and vitamin D, anti-resorptive therapies (bisphosphonates, SERMs, Denosumab, and calcitonin), and anabolic therapies (PTH analogs and sclerostin inhibitors). Appropriate nutrition, exercise, limited alcohol intake, and smoking cessation are also beneficial to promote bone health and reduce fracture risk [Table 2]. Understanding the factors contributing to osteoporosis and accurate diagnosis and effective management are necessary for orthopedic surgeons.
Declaration of conflict of interest
The author(s) do NOT have any potential conflicts of interest for this manuscript.’
Declaration of funding
The author(s) received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
No ethical approval was required for this study
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.