INTRODUCTION
Cartilage neoplasms exist along a spectrum, from benign enchondroma to high-grade malignant chondrosarcoma. Benign cartilage tumors, called enchondromas, are considered “Grade 0” lesions. As the grade of tumors increases, the degree of malignancy continues to rise: Grade 1 chondrosarcomas carry approximately a 5% chance of metastasis; Grade 2 chondrosarcomas metastasize up to 20% of the time, and Grade 3 chondrosarcomas metastasize up to 40-50% of the time.1 The histologic diagnosis of enchondroma versus Grade 1 chondrosarcoma is challenging due to subtle differences that may be indistinguishable on standard hematoxylin and eosin (H&E) examination.1 Because of this “gray zone” between Grade 0 and Grade 1 lesions, many times, these tumors are diagnosed as “atypical cartilaginous neoplasms” or CLUMPS (cartilaginous lesions of unknown malignant potential).1,2 Similarly, there have been conflicting reports about the role of magnetic resonance imaging (MRI) and other imaging modalities in distinguishing enchondromas from low-grade chondrosarcomas.1,2 In the absence of clear diagnostic criteria on histopathology and imaging, decision-making between Grade 0 and Grade 1 tumors is based on a consensus decision between radiology, histopathology, and clinical findings.1 However, this approach may result in potential over- or underdiagnosing of chondrosarcomas based on the different diagnostic criteria.1 Investigating techniques to improve diagnostic capabilities is critical because of the distinction in management between the two lesion types. Enchondromas do not require surgical intervention unless symptomatic, while Grade 1 chondrosarcomas (and higher) are treated with surgical excision.2
To address this diagnostic challenge, the Ki-67 index may be considered. Protein Ki-67 is a cell nuclear marker of mitotic proliferation, and it is assayed using an immunohistochemical stain on tumor tissue samples.3,4 The Ki-67 index quantifies the ratio of stained nuclei to all nuclei.3 Higher Ki-67 indices imply a higher proliferation rate of the cell population and thus is used as a proxy for evaluating tumor aggressiveness.4 This index has been researched for other cancers, such as breast tumors.5 For gastroenteropancreatic neuroendocrine neoplasms, the World Health Organization (WHO) lists the Ki-67 index as one of the factors included in the prognostic evaluation of these tumors.6
This retrospective pilot study aimed to determine if there is an association between cartilage tumor grade and the Ki-67 index and to evaluate its potential as an adjunct tool for distinguishing between critical cartilage tumor grades.
METHODS
Our institutional musculoskeletal oncology database was queried to identify all patients treated for cartilage neoplasms between 2010 and 2020. Considering the limitations of this pilot study, 26 patients were selected based on inclusion and exclusion criteria, representing a variety of tumor grades and depending on the quality and availability of formalin-fixed, paraffin-embedded (FFPE) retrievable tumor specimens. Patients were only included if the cartilage tumor did not represent a recurrence, metastasis of other cancer, or in the setting of genetic cause (e.g., Ollier’s syndrome, Maffucci’s syndrome). Clinical progress notes, imaging reports, and pathology reports from either biopsy or surgical excision specimens were referenced to establish the histological grading of each tumor. Our institutional practice is to categorize a cartilage tumor as a Grade 1 chondrosarcoma if the H&E staining demonstrated slightly increased cellularity (which is admittedly difficult to appreciate), entrapment of the bony trabeculae by cartilage matrix, or “nosing” of cartilage matrix and chondrocytes into the endosteal bone.
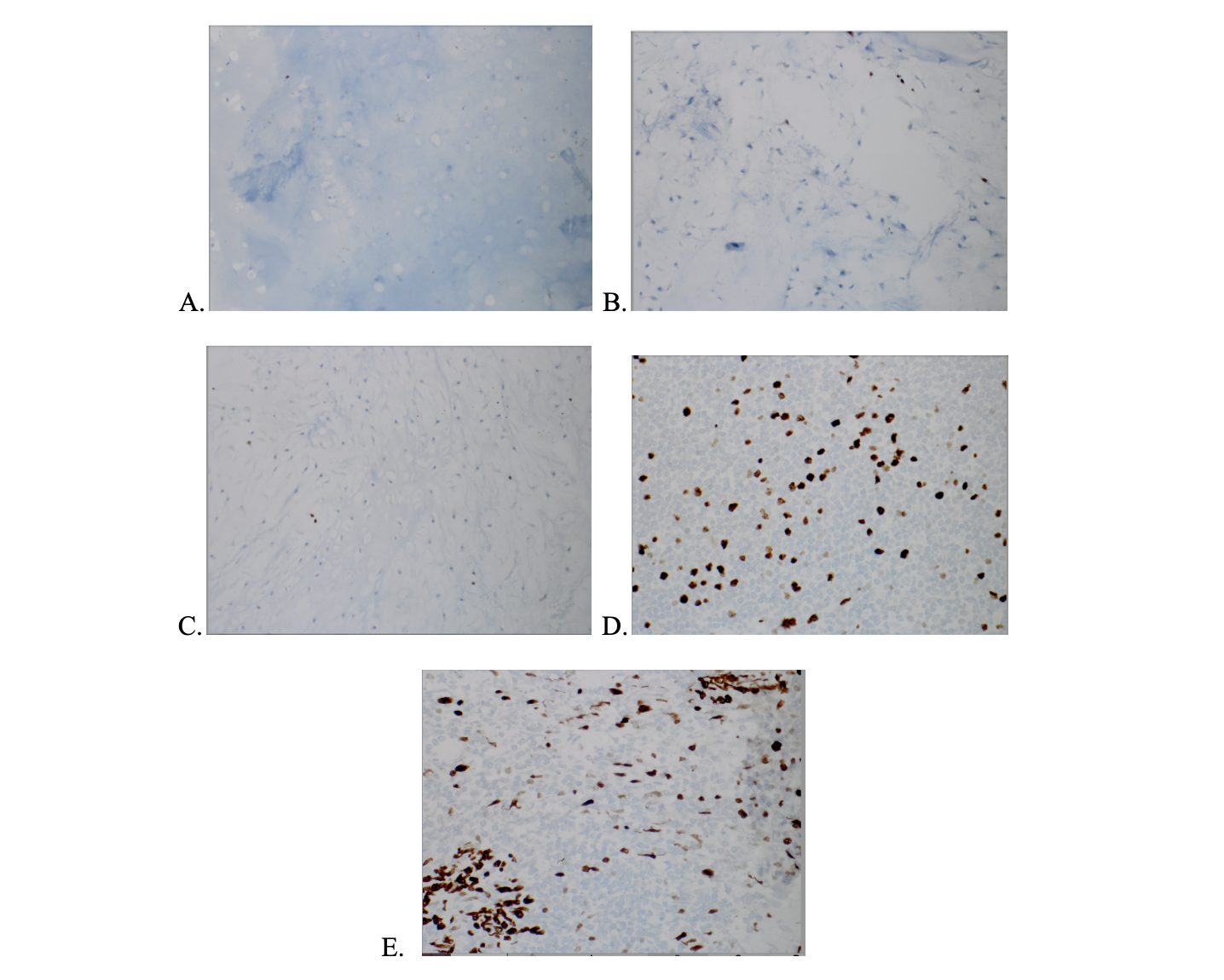
Ki-67 immunohistochemical stain was performed on the BenchMark ULTRA auto-staining system (Roche Diagnostics, Indianapolis, IN) using anti-Ki-67 rabbit monoclonal antibody (clone 30-9) and hematoxylin counterstain. Nuclei that were Ki-67 positive were stained brown, while those that were Ki-67 negative were stained blue. Ki-67 index was calculated by photographing and counting two high power fields with the greatest density of total stained nuclei (brown and blue stained nuclei, hotspot area) using ImageJ.7 Each region was independently counted by two observers, with a 95% intraclass correlation coefficient (ICC) [Figure 1A-E].
The Ki-67 indices for each tumor were statistically analyzed using Pearson’s correlation coefficient and one-way analysis of variance. Tukey’s honest significance post-hoc test and receiver operator curve were performed to examine further the Ki-67 index amongst grade 0 and grade 1 tumor subgroups. These analyses were performed using SPSS 27 (IBM, Armonk, NY).

RESULTS
Of the sample of 26 patients, the average age was 56 years. Lower extremity lesions comprised 69% of cartilage tumors [Table 1]. A greater average percentage of nuclei were Ki-67 positive in more advanced grades. [Table 1]. There was a strong positive correlation between tumor grade and the Ki-67 index (r = 0.704, p<0.001).
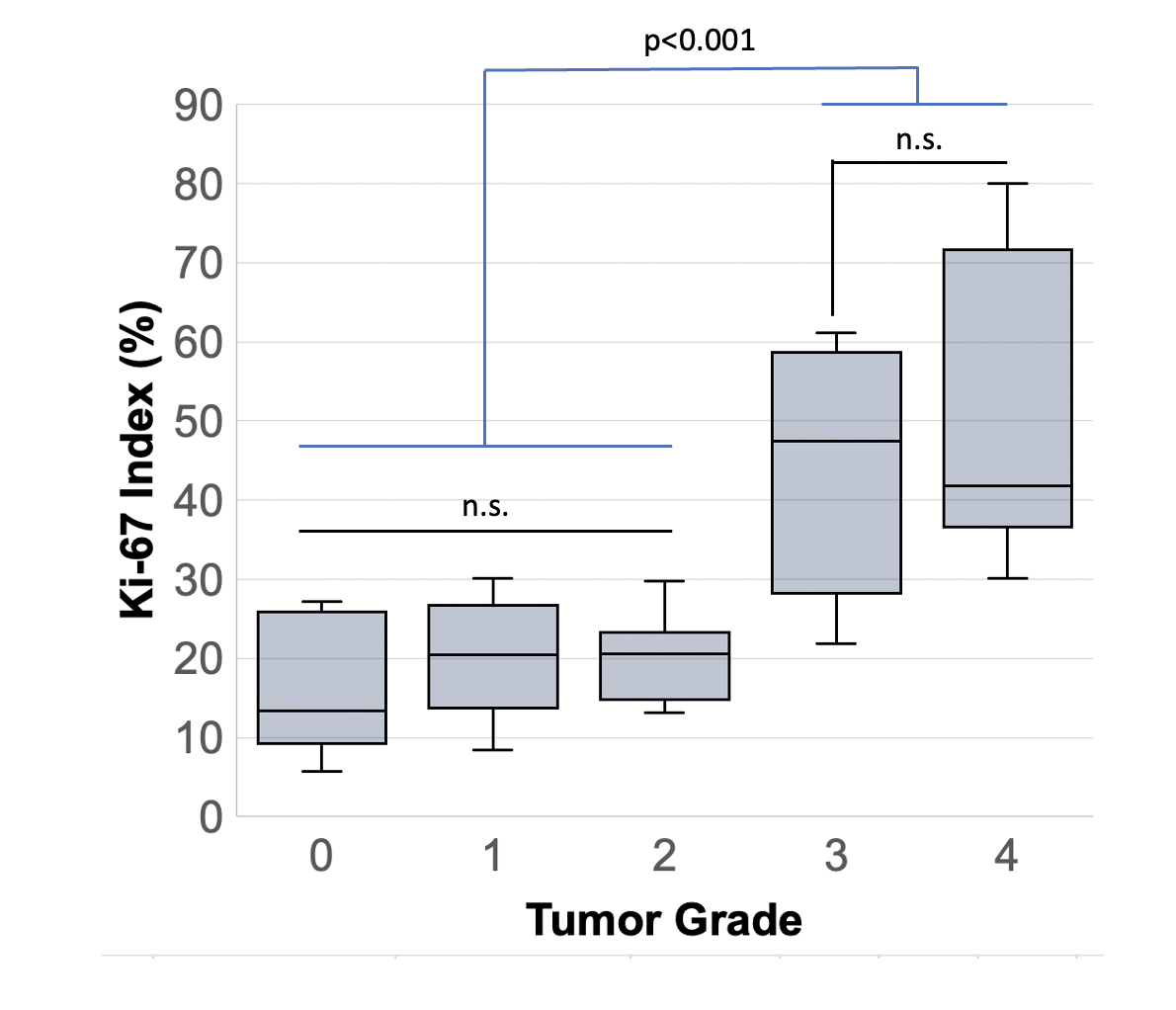
One-way ANOVA determined that there were significant differences in the Ki-67 index between grades (P<0.001) with strong interrater reliability (ICC=0.949). Tukey’s post-hoc test demonstrated that enchondromas were not significantly different from grade 1 cartilage tumor Ki-67 indexes (P=0.094). Enchondromas, grade 1, and grade 2 cartilage tumor Ki-67 indexes did not significantly differ from each other (0.094<P<1.000 for all pairwise comparisons). There was no significant difference between grade 3 and grade 4 cartilage tumor Ki-67 indexes (P=0.737). There was a significant difference between lower grade (0, 1, and 2) and higher grade (3 and 4) cartilage tumor Ki-67 indexes (P<0.001 for pairwise comparisons) [Figure 2].

A receiver operator curve (ROC) yielded an estimated cutoff index value of 13.4%, for which index values greater than 13.4% correlated with grade 1 tumors while index values less than 13.4% correlated with enchondromas. This cutoff was able to differentiate grade 0 vs. grade 1 with 67.9% sensitivity and 42.9% specificity.
DISCUSSION
This pilot study achieved proof of concept that the Ki-67 index can be calculated for cartilage tumors, and there is a positive correlation between Ki-67 and tumor grade overall (when evaluating grades 0-4). The difference in the Ki-67 indexes between grades 0 and 1 was not statistically significant, although we did find a trend towards a difference, and the ROC analysis established a cutoff Ki-67 value of 13.4% with decent sensitivity. The specificity of this cutoff value is only 42.9%; however, therefore the authors caution the reader that applying this cutoff value without evaluation of the tumor’s other characteristics may lead to over-diagnosis of Grade 1 chondrosarcomas and resultant over-treatment of benign lesions.
The blurry and indefinite distinction between these two lesions has been well-described in previous literature and supports the recent establishment of the entity known as “atypical cartilaginous neoplasms,” which is an attempt to describe tumors that exist along the spectrum between benign enchondromas and low-grade chondrosarcomas.2,8 Our findings should be considered in the context of these recent studies and serve as support for the inception of this entity. Furthermore, our findings should serve as early pilot data to charge future larger studies that may be more adequately powered to detect a small difference between the average Ki67 index of enchondromas and that of cartilage tumors with malignant potential (if one does truly exist).
Several limitations to this study restricted our ability to detect a difference if one truly does exist. A small sample size (n=26) may have limited the power of this study, contributing to a potential Type 2 error. By increasing the sample size, particularly of enchondromas and Grade 1 lesions, the study may have been powered to detect a subtle difference with statistical significance and improved the sensitivity and specificity of the cutoff value we calculated for the Ki-67 index that could be used to distinguish these two tumors. Patients were selected from a limited cohort secondary to inclusion criteria, availability, and quality; this may contribute to selection bias and somewhat limit the generalizability of our results. In particular, only somewhat-suspicious enchondromas undergo biopsy or excisional curettage. The surgeon’s suspicion is based on clinical behavior (e.g., bone pain at the tumor site) or concerning radiographic findings (i.e., growth, endosteal scalloping, cortical thinning, expansion, intralesional lysis). All enchondromas that did not meet the former were usually observed with imaging alone without obtaining tissue. Therefore, this is a source of bias in our study toward Grade 0 tumors being slightly unrepresentative of all Grade 0 tumors. This contributes to a lack of generalizability and could lead to a failure to detect a difference between their Ki67 index and the Grade 1 lesions.
Furthermore, the retrospective nature of this study relied on previously prepared tissue blocks of variable conditions from a 10-year time span, in which the method, quality, and consistency of tissue preparation could not be guaranteed on a patient-to-patient basis. For example, throughout the tissue review process, decalcified samples presented a challenge due to the incompatibility with the Ki-67 rabbit monoclonal antibody and hematoxylin counterstain protocol. A prospective study using Ki-67 immunohistochemical stain on fresh tissue samples that followed a consistent preparation process would help reduce variability in tissue sample quality and usability for evaluating the Ki-67 index. Another area for improvement in the study is using a more comprehensive and automated counting method. Although there was strong interrater reliability (ICC=0.949) using the ImageJ software and self-counting, the counting was performed by two observers, which by default carries a risk of bias and subjectivity that should be limited as much as possible and can always be improved. In a large-scale study, a more robust counting system would most likely be required to ensure consistency and reliability of the data collection.
CONCLUSION
Overall, this pilot study provided a framework for additional research on the clinical utility of the Ki-67 index for grading cartilage tumors. The goals of demonstrating proof of concept and investigating the feasibility and clinical utility of the Ki-67 index were achieved. With an established association between index and tumor grade (among the overall spectrum of tumors, Grades 0-4), further investigation into determining a threshold to distinguish benign enchondroma from grade 1 chondrosarcoma/ACT would be fruitful to enhance the evaluation of patients with histological- and radiographically ambiguous cartilage tumors, particularly given the potential surgical implications for these patients.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript. The senior author (CJG) serves on the editorial board for Surgical Collective.
Declaration of funding
The study received funding from the Cooper Medical School Medical Student Summer Research Stipend (BS and MK).
Declaration of ethical approval for study
This study has been reviewed by the institutional review board (IRB 21-067) with a waiver of informed consent on April 18, 2021.
Declaration of informed consent
No information in the manuscript can be used to identify patients.
Acknowledgments
We acknowledge Ms. Tara Coombs, Ms. Jacquelyn Gerhart, and Ms. Danielle Zaccagni for their time aiding logistics and staining protocol.