



Introduction
Fractures of the capitellum and trochlea comprise only 6% of distal humeral fractures and 1% of fractures about the elbow.1 They are commonly accompanied by other injuries, most commonly of the radial head or lateral collateral ligament (LCL).2 The goal of treatment for these injuries is a stable internal fixation that permits an early range of motion. However, this can be difficult to achieve due to limited surgical windows, their articular nature, limited bone stock for fixation, and extension into the trochlea medially or condyles proximally. Aside from open reduction internal fixation (ORIF), alternative surgical treatment options include fragment excision and arthroscopic assisted reduction and fixation.3,4 Here, we detail our preferred approach to treat capitellum fractures, including, preoperative planning, surgical anatomy, surgical setup and technique for simple and complex fracture patterns, postoperative care, and potential complications.
Indications and Contraindications
Due to their intra-articular nature, tendency to block motion, and propensity for displacement, most coronal shear fractures of the distal humerus are indicated for operative treatment.
Nonoperative treatment with immobilization can be considered for non-displaced fractures in low-demand patients, those with pre-injury limited use of the affected elbow, and those at unacceptable medical risk for surgery. Concurrent radial head and collateral ligament injuries are common, with reported rates of 11-54% and up to 48%, respectively, and when present, may also require operative repair.5,6 Additionally, posterolateral capitellum fractures with or without radial head fractures, termed Osborn-Cotterill lesions, can both result from and lead to posterolateral rotatory elbow instability (PLRI) through the mechanical engagement of the elbow upon extension and supination.7–9 These can present delayed with chronic PLRI in elbow extension and indicate combined osseous and ligamentous reconstruction.
Surgical Anatomy
Lateral approaches are most frequently used to expose isolated capitellum fractures (FIGURE 1).

The primary blood supply to the capitellum is from the posterior perforating vessels, which enter at the posterior aspect of the distal humerus, and most surgeons, therefore, attempt to preserve these soft tissue attachments.10 The lateral approach can be performed through multiple intervals: by elevating the anconeus and supinator from the subcutaneous border of the ulna (Boyd),11 by splitting the extensor digitorum communis [EDC] (Hotchkiss),12 between EDC and the extensor carpi radialis longus/brevis [ECRL/B] (Kaplan),13 or between the anconeus and the extensor carpi ulnaris [ECU] (Kocher).14 However, management of the LCL complex is a key portion of the lateral approach irrespective of the muscular interval utilized. This ligamentous complex originates from the lateral epicondyle deep to the extensor-supinator origin. It consists of the radial collateral ligament, lateral ulnar collateral ligament (LUCL), and accessory lateral collateral ligaments. The LUCL spans from the lateral epicondyle to the supinator crest, a tuberosity on the lateral ulna distal to the coronoid, and acts as the primary stabilizer of the ulnohumeral joint to varus stress.15 The Kaplan interval has been popularized to preserve the LCL while providing good lateral and anterior exposure of the capitellum. Unfortunately, with an intact lateral collateral ligament and radial head, it is difficult to visualize the anterior surface of the capitellum to reduce the fractured fragments and insert anteriorly-based orthopaedic hardware. Although it is best to keep the LCL intact during the procedure, if necessary, the LCL can be taken off of the lateral condyle sharply and repaired with drill holes or suture anchors upon closure.14 Alternatively, the LCL can be taken off with some lateral condyle bone with an osteotome or micro-sagittal saw and then repaired with internal fixation upon closure.16
Alternatively, an olecranon osteotomy will provide maximal exposure to a capitellum fracture when there is articular comminution, trochlear involvement, or proximal condylar extension. Through this approach, a direct or indirect reduction can be performed, posterior-to-anterior or anterior-to-posterior headless compression screws can be employed, and a posterolateral plate can be used to re-establish the posterolateral column is also involved. Upon closure, the olecranon osteotomy can be fixed with a plate, tension band construct, or intramedullary screw fixation (FIGURE 2).

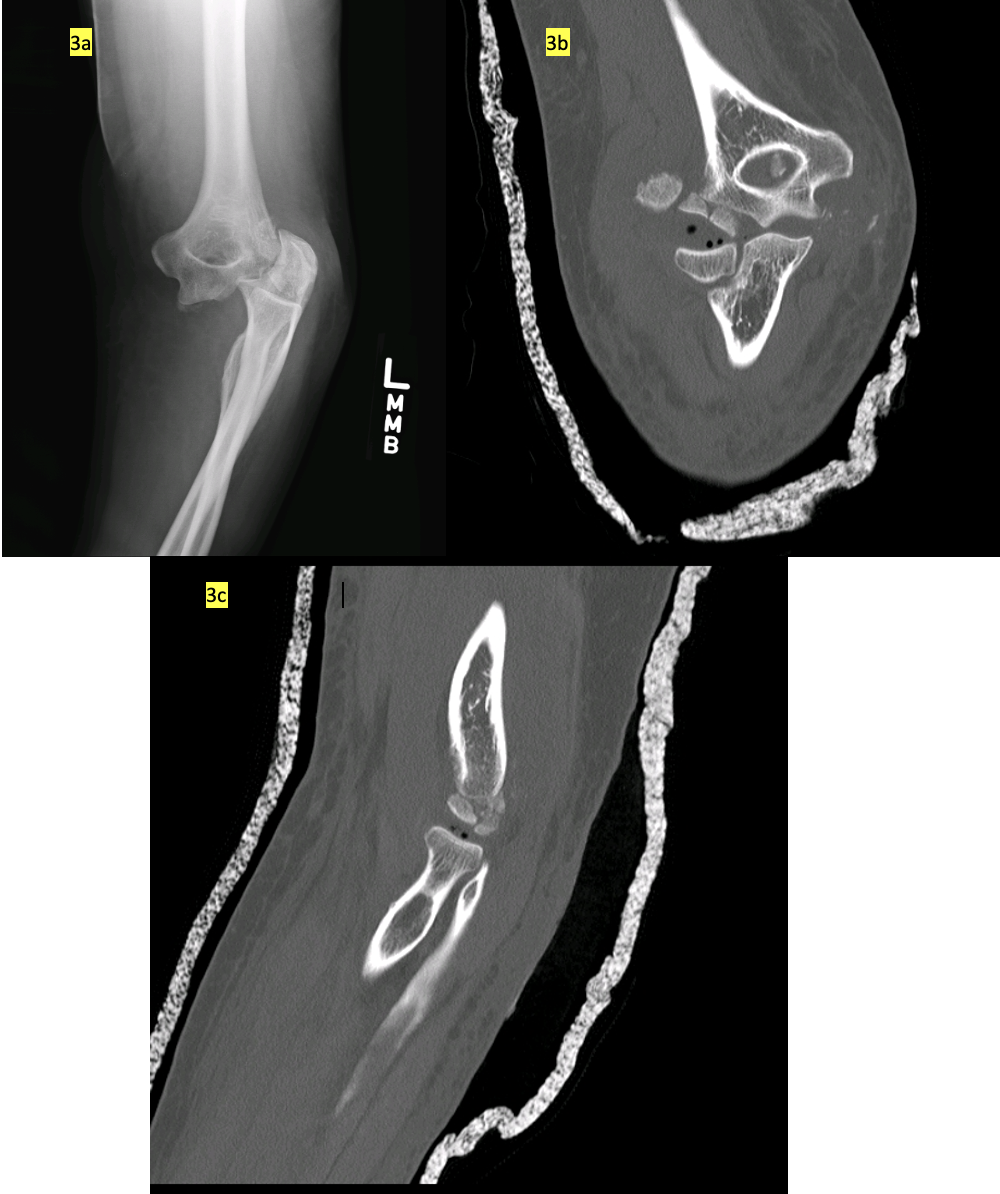
There are multiple fracture classifications in use, including the Kocher-Lorenz / Stein-Leventhal, the Bryan/Morrey/McKee, AO Foundation/Orthopaedic Trauma Association (OTA/AO), Ring, and Dubberly classifications.17–23 The latter is meant to guide management, with type 1 fractures involving the capitellum with or without the lateral trochlea managed with a muscle-splitting approach and ORIF, type 2 fractures with the capitellum and trochlea in one fragment managed with an extensile medial approach, and type 3 fractures with comminution of the capitellum and trochlea managed with olecranon osteotomy for exposure/fixation. The system includes an A or B modifier to classify the posterior condylar bone stock as simple or comminuted, which may necessitate bone grafting or plating24 (FIGURE 3).

Surgical Technique
Computed tomography (CT), with 3-dimensional (3D) reconstruction when accessible, is helpful for preoperative planning. We recommend general anesthesia or regional anesthesia with sterile tourniquet hemostasis. Necessary internal fixation includes 2.5 mm or 3.0 mm headless compression screws. In addition, if extension into the lateral condyle is suspected or present, locking lateral column plates should be available. If posterior comminution is present, patients should be consented to and prepped for autograft harvest, or allograft should be available.
Capitellum Fractures
A straight lateral approach is utilized with the patient kept supine for isolated displaced capitellum fracture without comminution, lateral condylar extension, or articular extension into the trochlea. Kaplan’s interval between EDC and ECRL/ECRB is utilized. Once the arthrotomy is performed, ready access and visualization of the displaced capitellum fracture should be evident. (FIGURE 1) The exposure can be increased by elevating the anterior half of the common extensor origin and brachioradialis proximally off the supracondylar ridge. Additional exposure can be achieved with elevation of the LCL complex posteriorly, followed by repair with suture anchors upon closure. Once exposed, the fracture can be readily reduced and provisionally fixed anterior to posterior, with the guidewires correlating to the cannulated headless compression screws intended for fixation. Two to three screws are recommended for adequate fixation and stability against shear and rotation of the fracture.
_headless_screw_fixation_of_a_capitellum_fracture_using_multiple_headless_compression.png)
Assuming adequate fracture reduction, stable internal fixation, and good integrity of the LCL complex, early motion can be instituted. If compromise of the LCL complex is determined based on the injury and/or during the exposure, it can be repaired or reinforced with a suture anchor.
Capitellar-Trochlear Shear Fractures
An extensile approach using an olecranon osteotomy is utilized for displaced capitellum fracture with comminution, lateral condylar extension, or medial articular extension into the trochlea. The patient is positioned lateral or prone to allow easier access to the posterior elbow. (FIGURE 5a) A straight universal posterior incision is utilized with full-thickness flap elevation.
_headless_compression_screw_fixation_of_a_capitellar-trochlear_shear_fracture_through.png)
The ulnar nerve is identified behind the medial epicondyle and protected throughout the case but not routinely transposed.
The osteotomy is performed first to facilitate exposure and fixation of the fracture. The triceps tendon is sharply mobilized on both sides, exposing the ulnohumeral articulation for the site of olecranon osteotomy. For later fixation of the osteotomy, a 6.5 partially threaded cannulated screw is prepared by placing the guidewire into a central position across the proximal ulna, followed by its over-drilling, tapping, and lastly measurement of optimal screw length for ultimate screw placement upon osteotomy closure. (FIGURE 5b) Next, with a micro-sagittal saw, a chevron olecranon osteotomy is performed at the level of the ulnohumeral joint to the level of the subchondral bone. (FIGURE 5c) The final cut into the joint is performed carefully with an osteotome to minimize thermal injury to the articular surface and to allow an irregular surface for interdigitation upon closure. Once the osteotomy has been performed, the fracture is examined (FIGURE 5d), debrided, mobilized, reduced, and provisionally held with the guidewires correlating to the cannulated headless compression screws planned for fixation. (FIGURE 5e) With the fracture reduced, it is internally fixed with multiple headless compression screws placed in parallel (FIGURE 5f) while ensuring the screw is not prominent on either side of the articular surface. (FIGURE 5g) With the fracture repaired, the osteotomy site is closed by placing the previously measured 6.5 partially threaded cannulated screw through the pre-drilled path by reducing the osteotomy and placement of its guidewire. (FIGURE 5h) Assuming adequate fracture stability, early motion can be instituted post-operatively.
Post-operative care
The stability of fixation and the status of the LCL largely dictates the postoperative course. If the ligament was repaired during surgery, it should be protected, but early active motion is still preferred. Based on perceived stability intraoperatively, we recommend a short course of immobilization at 60-90 degrees of flexion for 2-14 days before beginning the range of motion. Post-operative external beam radiation or six weeks of indomethacin can also be considered for heterotopic ossification (HO) prophylaxis.
Pearls and Pitfalls
We find the best internal fixation options for capitellum fractures are headless compression screws. Alternatively, if there is either posterior comminution or proximal condylar extension, we find the use of a posterolateral locking plate to be beneficial in stabilizing the lateral column while restoring the posterior buttress while facilitating posterior-to-anterior locking screw fixation of the capitellum fracture. Alternative internal fixation options include biodegradable pins and headed posteroanterior cancellous lag screws. However, small articular fragments that cannot accommodate fixation can be excised to prevent them from becoming intra-articular loose bodies.
Capitellum fractures can sometimes occur in the setting of complex elbow instability. While hinged external fixation can permit early motion when instability persists after repair of all osseous and ligamentous injuries, we prefer temporary internal bridge fixation of the elbow at 90 degrees with a posterior plate spanning the humerus and ulna when instability is present. This technique allows for stable reduction of the ulnohumeral joint to permit soft tissue healing of the ligamentous complexes medially and laterally. This plate is then removed 4-6 weeks post-operatively, and gentle manipulation under anesthesia is performed at the time of removal.25
In low-demand patients of advanced age who are still surgical candidates, particularly with articular comminution or loss of lateral humeral bone stock, hemi or total elbow arthroplasty should be considered as an alternative to ORIF.26
Complications
Surgically treated capitellum fractures can be complicated by stiffness, osteonecrosis of the capitellum, nonunion, malunion, instability, heterotopic ossification, post-traumatic arthritis, ulnar or radial neuropathy, and complex regional pain syndrome (CRPS).27–29 Complications are common following these injuries, and patients should be counseled about such pre-operatively.
Postoperative stiffness and impingement are common and may be more prevalent in Dubberly type B fractures where a posterior plate was utilized. If stiffness persists following a course of therapy, surgical treatment can be offered as hardware removal and capsulectomy.
Options for treating painful malunion or capitellar osteonecrosis include fragment excision, revision ORIF, corrective osteotomy, or arthroplasty. Arthroplasty may include resurfacing capitellar hemiarthroplasty, resurfacing radiocapitellar arthroplasty, distal humeral hemiarthroplasty, and total elbow arthroplasty.30
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.’
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
Not applicable
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.