Introduction
Since the earliest recorded medical texts, the management of fractures of the proximal humerus has challenged physicians.1 The management recommendations for non-operative reduction established by ancient Romans and Greek medical authorities remained unchanged through medieval and early modern medicine consisting primarily of the Hippocratic mode of reduction by forceful extension and manipulation followed by bandaging and delayed splinting.2,3 The methods of reduction were largely non-operative until the nineteenth century with the introduction of ether anesthetics in 1846, antiseptic surgical methods in 1867, and Rontgen’s discovery of the X-Ray in 1895.2 Subsequently, although unpopular at the time, American surgeon Samuel D. Gross recommended open reduction of proximal humerus fractures in his 1862 textbook, “…cut down upon the dislocated bone, and push it back into its natural position. The broken pieces being placed in contact, and the wound carefully closed, I should not apprehend any bad results from inflammation and its consequences”.4 Although we are now in a time of advanced diagnostic and operative technologies, controversies regarding the optimal treatment of complex fractures of the proximal humerus still persist.
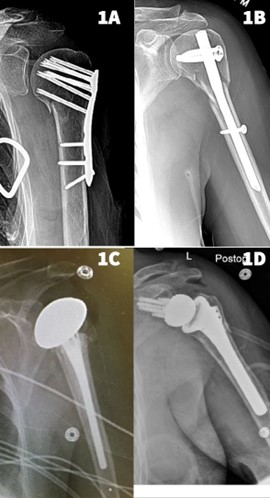
Fractures of the proximal humerus are the third most common upper extremity fractures in the United States and account for 5-6% of all adult fractures.5 These injuries have a bimodal distribution involving young patients with high-energy trauma or, more commonly, older patients with low-energy falls. Studies that focused exclusively on non-operative treatment yielded a 98% rate of radiographic union. Still, these results are offset by a high overall complication rate of 48%, including varus malunion and osteonecrosis.6 Operative treatment options for proximal humerus fractures include percutaneous pinning, open reduction and internal fixation (ORIF), intramedullary nails (IMN), hemiarthroplasty (HA), and reverse total shoulder arthroplasty (rTSA). [Figure 1] This review will focus on the latest evidence and outcomes following non-operative and operative treatment of proximal humerus fractures (PHF).

Classification of Fractures
The utility of fracture classifications is their ability to guide treatment and inform prognosis while maintaining high inter-observer reliability. Unfortunately, proximal humerus fracture classifications have historically had low inter-observer reliability.7 Moreover, several variables affect outcomes following proximal humerus fractures beyond fracture characteristics, including patient age, comorbidities, bone quality, and associated injuries. However, the two most commonly referenced classifications include the Neer and Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA) classifications.
Neer Classification
The most commonly used classification of proximal humerus fractures is the Neer classification.8 Neer based this classification system on the anatomic relationship of four segments on plain radiographs: the greater tuberosity, lesser tuberosity, articular surface (anatomic head), and humeral shaft. Beyond these four segments being defined by the fracture line, they are only considered a ‘part’ if displaced greater than 1 cm or if there is greater than 45 degrees of angulation. Fractures that do not meet the criteria for displacement are considered ‘undisplaced’ or one part. Two-part, three-part, and four-part fractures involve displacement of some or all the previously mentioned segments. A meta-analysis reported an inverse correlation between Constant-Murley clinical outcome scores and the number of fracture parts supporting the use of this classification.9
AO/OTA Classification
The AO/OTA classification includes three main fracture types (A, B, C), which are further divided into three subgroups based on the degree of displacement, impaction, and dislocation of the fractured fragment, each with three further subgroups yielding a total of 27 fracture subtypes. Type A fractures are “extra-articular, unifocal, with intact vascular supply”; type B fractures are “extra-articular, bifocal, with possible vascular compromise”; and type C fractures are “articular, with a high likelihood of vascular compromise”.10
In 2018, the AO/OTA introduced a new fracture and dislocation compendium addressing the criticisms of the existing classification and simplifying the coding process.11 The new classification system integrates Neer’s criteria into the fracture description and consists of 13 fracture subgroups. The new AO/OTA 2018 classification was found to significantly improve the agreement of observers’ reliability and reproducibility compared with the AO/OTA 2007 system.11
Operative versus Non-operative treatment
Proximal humerus fractures can be treated non-operatively whenever possible, particularly with non- or minimally displaced fractures. In 2016, Han et al. reported that non-operative treatment was the most common treatment of proximal humerus fractures in older people.12 When surgery is indicated, open reduction and internal fixation with a plate and screw construct has historically been the most common operative procedure. However, reverse total shoulder arthroplasty (rTSA) rates for proximal humerus fractures are increasing.5
In 2015, the ProFHER (Proximal Fracture of the Humerus: Evaluation by Randomization) Trial reviewed 250 patients randomized to non-operative or operative treatment and matched by Neer fracture type with 2- and 5-year follow-up.13 There was no statistically or clinically significant difference between operative vs. non-operative Oxford Shoulder Score (OSS) (39.07 vs. 38.32) or SF-12 (37.3-40.76 vs. 36.57-39.99).13 In addition, there were no significant differences in secondary outcomes such as health-related quality of life, complications related to surgery, secondary surgery, and mortality.13 Of the operative group complications (30/125; 24%), the most common were hardware issues (10/30; 33.3%) and posttraumatic stiffness (6/30; 20%). In the non-operative group, complications (23/125; 18%), the most common were symptomatic malunion (5/23; 21.7%), nonunion (5/23; 21.7%), and posttraumatic stiffness (5/23; 21.7%). Of note, 11 participants in each group required secondary surgery. Despite supporting non-operative treatment, this trial excluded PHFs in which the authors deemed operative intervention necessary, limiting its findings. It is known that salvage surgery following initial non-operative treatment yields poorer outcomes in functionality and pain as compared to initial operative treatment.14
A Cochrane review of six heterogeneous trials with a total of 270 participants evaluated operative versus non-operative treatment for PHF.14 Pooled results found no statistical difference between patient-reported functional scores of the two groups.14 Pooled DASH scores showed no statistically significant difference at any time up to 2 years, although there was a potential trend to a more favorable result after surgery.14 Also, no statistically significant difference was found between the two groups in American Shoulder and Elbow Surgeons (ASES) scores at one year. Secondary surgeries were greater in the operative group (16%) than in the non-operative group (4.5%). When examined radiographically, there was no significant difference in nonunion, osteonecrosis, and signs of osteoarthritis.
Two-Part Fractures
In 2019, a prospective randomized controlled trial of 88 patients with displaced two-part PHFs found no evidence that operative treatment is superior to non-operative treatment at a 2-year follow-up.15 There was also no significant difference in complication rates in the operative group (3/88; 6.8%) and non-operative group (0/44; 0.0%). Two operative complications were due to implant failures because of proximal screw migration and one due to a fall.
Three-Part & Four-Part Fractures
Many studies have demonstrated no difference in outcomes between non-operative treatment versus common operative options such as ORIF, HA, and rTSA.16 However, non-operative treatment in older adults with osteoporotic bone leads to compromised outcomes with early failures, especially in three- and four-part fractures.13,14 The literature has demonstrated that rTSA is superior to ORIF and HA for three- and four-part fractures in elderly patients with osteoporotic bone.17
Recent studies have now begun examining rTSA versus non-operative treatment in elderly patients.18 Chivot et al. compared rTSA (n= 28) to non-operative (n= 32) treatment in three- and four-part fractures with a minimum of 2-year follow-up and found a statistically significantly improvement on functional outcomes using the Constant score in rTSA patients, but the clinical difference was minor.18
Operative Treatment Outcomes
Discrepancies continue to exist in displaced PHFs concerning operative versus non-operative management. Generally displaced three or four-part fractures are indicated for operative fixation, although the ProFHER trial demonstrated satisfactory results may be achieved when PHFs are managed non-operatively.13
Open Reduction Internal Fixation
ORIF of a displaced PHF usually consists of open fracture reduction and fixation with a periarticular locking plate on the lateral aspect of the humerus. It can be performed through a deltopectoral or lateral deltoid splitting approach. The goal of ORIF is anatomic reduction of the fracture, restoration of normal humeral head and neck angle, tuberosity and/or rotator cuff repair, and early return to motion.
Buchmann et al. evaluated functional outcomes following ORIF in 149 patients with AO/OTA type B PHFs with a minimum of 1-year follow-up.19 Complications were reported in 15 patients (10.1%). Five patients had transient postoperative nerve injury, three of the axillary and two of the radial nerve. Six patients had soft tissue complications without detailed elaboration. The remaining four complications required re-operation for screw perforation and secondary humeral head osteonecrosis. In addition, 26 patients (17.5%) had signs of radiologic nonunion 12 months after surgery. The average range of motion was 82.2° of abduction and 115° of forward flexion.
Dabija et al. evaluated database outcomes of 134,411 patients with proximal humerus fractures treated non-operatively (n=121,411), ORIF (n=8,994), or with arthroplasty (n=4006).20 Patients who underwent ORIF were significantly more likely to have wound complications than those who underwent an arthroplasty. The differences in rates of revision surgery between patients treated non-operatively (9,157/121,411; 7.6%), with ORIF (594/8994; 6.6%), and with arthroplasty (290/4006; 7.2%) were similar. Among ORIF patients, 2.5% (n= 225) underwent a revision ORIF, and 4.1% (n= 369) ultimately underwent an arthroplasty.20 In contrast, in patients initially treated non-operatively, 4.5% (n= 5410) underwent secondary ORIF, and 3.1% (n= 3747) underwent an arthroplasty.20 Of patients initially treated with arthroplasty, 1.8% (n= 73) underwent revision ORIF and 5.4% (n=217) underwent a secondary arthroplasty.
Fleischhacker et al. evaluated the malposition of humeral head to shaft following ORIF in 685 patients with two-year follow-up21. Functional outcomes measured by Constant scores were inferior in a humeral head-shaft angle of 10-20° varus relative to an anatomical angle of 135°. Functional outcomes further deteriorated with varus malposition of >20°. These study findings emphasized the importance of restoring the anatomic alignment of the humeral head and avoiding residual varus alignment following the ORIF of the PHF.
Intramedullary Nailing
IMN fixation potentially allows for fracture repair in a minimally invasive fashion, minimizing disruption of vascularity and internal fixation with a load-sharing device.22 The utility of IMN in all types of PHFs is still debatable. Generally, it is recommended in elderly patients to treat displaced simple fracture types such as two-part or three-part with a sufficient subchondral bone bridge lateral to the nail’s tip at the top of the head.
Wong et al. systematically reviewed 14 studies (10 retrospective, 4 prospective) with 448 patients with two-, three-, and four-part PHFs managed with IM nail fixation.23 They reported an overall mean Constant score of 72.8 with an ASES score of 84.3 postoperatively. The most common complication reported was secondary loss of reduction in 24% and malunion in 21% of patients. The reoperation rate was more common in four-part fractures at 63.2% compared to 13.6% and 17.4% in two- and three-part fractures, respectively.23
Studies comparing IMN directly to plate fixation found somewhat similar outcomes.24 Guo et al. reported IMN is less invasive compared to ORIF based on operation time and intra-operative blood loss but takes longer to achieve fracture reduction and fixation.24 However, no significant difference was identified between shoulder function VAS and Constant-Murley scores between the two cohorts.
Hemi-arthroplasty
HA is generally indicated for displaced three- or four-part PHF with displaced anatomic heads or head-split fractures. The prosthesis can be press fit and/or cemented and allows for early return to motion, but requires intact or adequately repaired tuberosities to maximize outcomes. Incompetent tuberosities, a torn or incompetent rotator cuff, and pre-injury rotator cuff arthropathy are relative contraindications to HA. Despite the relative success of HA for proximal humerus fractures, rTSA has become the arthroplasty treatment of choice for proximal humerus fractures.
The literature supports that HA is the inferior arthroplasty option regarding the range of motion, patient-reported outcome measures, and revision rates following PHFs. A prospective RCT of 31 HAs found an increase in Constant scores, forward elevation, and abduction post-operatively but all significantly lower than rTSA.25 HA patients with failure of the tuberosity healing had significantly worse mean Constant scores (21.4 vs. 51.2; P = .001), active forward elevation (52.7 vs. 100.6; P = .001), and abduction (54.6 vs 94.0; P = .001) compared to those which had healed.
Reverse Total Shoulder Arthroplasty
RTSA has become increasingly popular in the United States (US) among elderly patients with PHF since its Food and Drug Administration (FDA) approval in 2004. The literature has exploded with data supporting rTSA’s improved functional outcomes and low reoperation rates over 2022 alone.26 Anatomic reconstruction is theoretically inferior to rTSA since the former relies on the rotator cuff muscles for power and arm positioning while the latter utilizes the deltoid muscles. Most elderly patients may have chronic rotator cuff arthropathies. Therefore rTSA becomes the most appropriate arthroplasty option.
The literature has demonstrated Constant scores between 44 and 68, active forward flexion between 97° and 123°, abduction between 97° and 113°, and external rotation of approximately 18°-25°.27 Jain et al. conducted a meta-analysis of 382 rTSA’s with a minimum follow-up of 24 months and concluded that healed tuberosities demonstrated an improved range of motion and outcome scores.28 Patients with healed tuberosities had superior active forward flexion (134.1° vs. 112.5°, P < 0.05), abduction (114.8 vs. 95.1 degrees, P < 0.05), external rotation (27.8 vs. 7.6 degrees), and mean Constant score (63.5 vs. 56.6, P < 0.05) than those with an unhealed tuberosity.28
RTSA has become the treatment of choice for PHFs that have failed nonoperative care, fixation, or HA, particularly when there is malunion or nonunion of the tuberosity. There is growing evidence of its use for elderly patients with fracture-dislocations and comminuted fractures.
Complications
Non-operative
The most common complications of non-operative treatment of PHFs are nonunion, malunion, osteonecrosis, or neurologic injury. Complications are higher when surgery is implemented after failed non-operative management than acute fractures are immediately treated operatively.13,14
A review of 650 patients with one-year minimum follow-up evaluating PHFs treated non-operatively reported 98% radiographic union and 13% complication rate.6 Varus malunion was the most common complication (7%), and osteonecrosis was relatively uncommon at a mere 2%.6 However, a more recent systematic review and meta-analysis directly analyzing the rate of osteonecrosis found a rate of 10% in PHFs treated non-operatively.29
Operative
The rate and type of operative complications largely vary depending on the surgical treatment, type of fracture, and surgeon experience. It has been reported that, on average, 5 % of proximal humerus fractures treated operatively will undergo additional surgery.13,30
A multicenter review of 898 operatively treated PHFs reported a 12.5% overall complication rate, a 5% revision rate, and a 6% mortality at one year postoperatively. The most common reasons for revision were instability (2.5%), peripheral nerve injury (1.3%), and infection (1.3%).30
The literature has also reported rates of osteonecrosis of 3.2% and hardware failure of 8%.13 Infection risk occurs at a rate between 0-4% in the literature.19,23,24,30
Conclusion
This review evaluates some of the latest evidence regarding the outcomes of PHFs when treated operatively and non-operatively. Many controversies remain about when to manage a PHF operatively or non-operatively. Non-operative treatment is generally recommended for non- or minimally displaced fractures or elderly low-demand patients. Intramedullary nail fixation is usually utilized for simpler fracture patterns, especially in two-part surgical neck fractures. Open reduction internal fixation with a locking plate and screw construct is preferred in younger, higher-demand patients with three- and four-part fractures, even if the injury has a head split component. Arthroplasty is reserved for older patients with three- and four-part fractures who are at risk for complications or failure of ORIF or are in low functional demand. Reverse total shoulder arthroplasty is preferred to hemiarthroplasty, given the more reliable treatment outcomes and less reliance on tuberosity healing for postoperative function.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
Approval not required.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.