

INTRODUCTION
In the realm of orthopaedic surgery, there are exceptionally few disease entities that are as poorly understood and devoid of evidence-based guidelines as there are with Charcot Neuroarthropathy (CN). Yet, the socioeconomic impact of the disease continues to be a tremendous cost to our healthcare system with minimal change in morbidity or mortality.1,2
As the rate of diabetic neuropathy increases, so will CN. A greater effort must be placed on understanding this disease and formulating treatment guidelines. Fortunately, over the last decade, there has been a steady increase in basic science research aimed at understanding the pathophysiology of this disease, and recently, our lab has published the first animal model that mimics the neurodegenerative human Charcot condition.3–5 Furthermore, several new surgical techniques and adjuvants have emerged in the surgical treatment for CN.6–8
While there is still a paucity of literature from which to form evidence-based practice guidelines, a summary of the most current knowledge will be beneficial in guiding future research in the hope of developing best practices for clinicians treating this disease. As such, the following topical review will highlight advances in the treatment and understanding of CN.
REVIEW
BACKGROUND & PATHOPHYSIOLOGY
CN of the lower extremity is a progressive, neurodegenerative disease that arises from the combination of peripheral neuropathy and trauma. CN can destroy foot anatomy, resulting in ulcers, infection, and even amputation.3 While the true prevalence of CN is unknown, estimates range from 0.1% to 10% among patients with diabetes. These values increase to 35% among patients with diabetes and peripheral neuropathy.9
CN is associated with high rates of morbidity and mortality. For example, a retrospective study evaluating outcomes of 173 CN patients found a mean survival of 12.7 years after the first diagnosis and a 14% 5-year mortality rate.10 This same study determined the complication frequency to be 63%, with 10% of patients requiring a major amputation.10 Furthermore, in patients that go on to require amputation, research has estimated 5-year mortality up to 55% and 74%.11,12
The leading hypothesis of the pathophysiology is developed around a neurovascular and neurotraumatic theory [Figure 1]. Peripheral neuropathy, abnormal neuropeptide release, trauma, and abnormalities in the microvasculature of the leg have been shown to increase blood flow, leading to a rise in venous pressure and subsequent enhanced capillary leak.13,14 This raises compartment pressure, which causes arteriovenous shunting and local ischemia, damaging the surrounding ligaments and joints.13,14

In addition, the repetitive acute and subacute trauma occurring secondarily to the loss of peripheral sensation initiates a reaction mediated by several proinflammatory cytokines. These cytokines promote excessive osteoclastogenesis and bone turnover by upregulating the receptor activator of nuclear factor-κB (RANK) and the receptor activator of nuclear factor-κB ligand (RANK-L). Moreover, repetitive trauma reduces anti-inflammatory cytokines, further perpetuating this cycle. This theory has been supported by several studies that have reported elevated levels of TNF-alpha, IL-6, and C-reactive protein in patients with CN.13,15
The current neurovascular and neurotraumatic theory has been supported by King et al., who developed a novel FEMASK-scoring system based on histopathological findings of CN.4 The FEMASK-scoring system uses a scale of 0,1,2,3, indicating distinctive intraneural arteriolosclerosis, the first stage of CN with large, embedded bone or cartilage fragments, the second stage showing mixed large and small bone fragments, and the end stage with complete absence or resorption of bone fragments, respectively. Their reproducible results demonstrate the pathogenesis of CN, and the scoring system will help surgeons determine adequate treatment that can be correlated to patient outcomes.
Apart from neurovascular and neurotraumatic theories, genetics may influence CN development.16 Mitchell et al. found fewer synovial mesenchymal stromal/stem cells in patients with CN than without. Pasquier et al. noted an altered expression profile of circulating miRNAs, and Guo et al. suggested that calcitonin gene-related peptide (CGRP) may also play an important role due to its ability to stimulate collagen degradation in vivo because higher rates of CGRP in the synovium of patients with CN were discovered.17–19 Lastly, there are alternative causes of Charcot other than diabetes, such as syphilis, alcoholism, B12 deficiency, and idiopathic.
PRESENTATION AND WORKUP
Early diagnosis of CN is difficult due to varied symptoms. However, any patient presenting with diabetic neuropathy and lower extremity swelling, pain, edema, redness, or deformity should be considered.3 Patients with CN who present acutely will have a temperature difference of at least 2°C compared to the contralateral unaffected side, and elevating the limb will resolve the redness and can easily differentiate CN from infection.3,9 Short et al. described that early and accurate imaging and a thorough history and physical exam are crucial for differentiating CN from osteomyelitis.20 Patients may present with severe foot deformities in the later stages due to metatarsal collapse and joint destruction. The loss of the medial longitudinal arch may cause the classic “rocker-bottom” deformity.21
For suspected CN, standard, weight-bearing, orthogonal radiographs of the foot and ankle with contralateral comparison views are essential to diagnose subtle and early collapse and to monitor progress, albeit radiographs may be normal during the early stage of the disease. Likewise, Magnetic Resonance Imaging (MRI) or computerized tomography (CT) scans for patients with contraindications can be ordered using a large field view to help confirm the disease, monitor progression, and evaluate response to treatment.22,23 However, MRI is limited in its ability to distinguish active CN from acute osteomyelitis.24 A recent meta-analysis concluded that while MRI, white-blood-cell scintigraphy, and positron emission tomography (PET) scans all have similar sensitivities for detecting osteomyelitis, PET scans have an overall higher specificity.25
While many physicians routinely obtain inflammatory markers, such as C-reactive protein (C-RP) erythrocyte sedimentation rate (ESR), these have little value in the diagnosis of CN due to their nonspecific nature. No specific biomarker has been identified for diagnostic purposes. Hemoglobin A1c (HbA1c) is a good indicator of glycemic control and should be obtained in diabetic patients, while vitamin B12 should be ordered for non-diabetic patients.26
After diagnosis, the Eihenholtz, Brodsky, or Sander-Frykberg classification may be used to guide treatment.27 At our institution, we have employed a combined approach utilizing the Eichenholtz staging combined with pathologic grading. This combined approach demonstrates strong correlations with predicting outcomes defined as preventing the progression of the disease and salvage amputations in Charcot patients.4 In addition, some consensus groups recommend using “active” and inactive" Charcot to clinically stage.28 Regardless of the classification system used, research has suggested all three can still be useful in helping with the diagnosis and management of CN.27
NONOPERATIVE TREATMENT
What is the goal of nonoperative treatment?
Nonoperative treatment aims to maintain a plantigrade foot, prevent the development of new ulcers, allow present ones to heal, enable the ability to weight bear with or without a brace and have the ability to wear diabetic shoes and maintain ambulation [Figure 2]. Total contact casting (TCC) remains the gold standard for nonoperative treatment, especially in the early stages. The length of time a patient will stay in a TCC will vary depending on the location of the deformity. Patients should generally remain in a TCC until osseous consolidation is achieved and after exiting the acute inflammatory phase. Following resolution, patients may be fitted for a Charcot Restraint Orthotic Walker (CROW), hoping to eventually progress to customized orthoses or transition to a boot and, ultimately, shoes with inserts.3

Has the traditional TCC evolved?
Recent research aims to enhance TCC methods to improve patient satisfaction and reduce skin complications.29,30 Removable cast walkers allow patients and physicians to perform regular skin examinations and modify the inner surface as needed.31,32 However, recent research has argued that irremovable TCC is more economical and leads to better healing and quality-adjusted life-years.31 Despite these findings, researchers have continued to explore ways to modify the traditional TCC to lessen skin complications and improve outcomes. Hopchlenert and Fischer recently created a bivalved TCC that allows only partial cast removal, creating a ventral window for viewing the foot.33 De Souza et al. demonstrated that for treatment of acute CN Eichenholtz stage 1, immobilization with TCC is safe and allows patients to bear weight.34 Much like removable cast walkers, their design allows physicians to perform regular wound checks while eliminating the risk of patient nonadherence.33
Are pharmaceutical agents effective?
Multiple pharmaceutical agents, such as bisphosphonates, calcitonin, and denosumab, have been proposed as possible treatments.35,36 Of these agents, bisphosphonates have been the most extensively studied, and there is limited evidence to support their use.37 Likewise, no studies have evaluated the effectiveness of daily intranasal calcitonin in improving patient-reported outcomes.38
More recently, Petrova et al. performed a randomized controlled study to assess the effect of recombinant human parathyroid hormone (PTH) on the resolution time of active CN.39 Unfortunately, their study concluded that there was no difference in time to resolution.39 However, additional studies have begun to investigate denosumab. In one observational study, fracture resolution time and time to clinical cessation were shorter in patients receiving denosumab.35 Furthermore, a level III open-label trial found that patients receiving denosumab exited the acute inflammatory phase at an average of 52 days following injection, suggesting that it may be beneficial.36 Overall, there is limited evidence to support the role of pharmacotherapy for earlier remission.40
OPERATIVE TREATMENT
What is the goal of operative treatment?
The goal of operative treatment is to obtain a stable, functional plantigrade foot, remove osteomyelitis, and prevent future ulceration and deformity. After determining surgical intervention is necessary, surgeons should work with other providers to optimize medical management after failing nonoperative management. In doing so, surgeons may consider using the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) risk calculator, which accurately predicts perioperative risk in CN patients undergoing reconstruction.41 In addition, on multivariable analysis, longer lengths of stay were associated with low preoperative hemoglobin values (rate ratio [RR], 1.36; P = 0.01) and congestive heart failure (RR, 1.42; P = 0.02). Optimization of patients with diabetes and multiple medical comorbidities before elective Charcot reconstruction allows the surgery to be performed with a predictable risk for perioperative complications.41
When is surgery indicated?
In general, operative treatment is appropriate for patients with limb or life-threatening infection, who fail conservative management, or those with substantial deformities who are not amenable to bracing.42 The optimal timing for surgery remains unclear. While it was traditionally not recommended to operate during the acute phase of the disease or in the setting of infection or ulceration, many experienced surgeons have challenged this belief.42 A recent study demonstrated that tibiotalocalcaneal arthrodesis could be effective in patients with active hindfoot ulceration.43 Most surgeons often operate on patients with active ulcers because the ulcers are slow to heal or recur quickly because of the deformity. Furthermore, Kavarthapu and Budair have had success utilizing a two-staged reconstruction method that does not require ulcer healing before proceeding to the second stage of internal fixation, which uses intramedullary nailing (IM) to stabilize the subtalar and ankle joints and a combination of lag screws, locking plates, and beams for the midfoot.44 While more studies are needed to explore intervention in the active phase, these few studies are promising. Although, surgeons should still use caution when deciding how to manage a patient with active ulceration. A recent study by Wukich et al. that evaluated 245 patients with CN reported that a CN-related wound at presentation increased the likelihood of major amputation by a factor of 6.45 Radiographic analysis in CN patients with ulceration can also be useful when stratifying the risk for both ulceration and the necessity for surgery.32,46 Nevertheless, surgical reconstruction has improved quality of life, necessitating further investigation into the optimal timing and indications.47
How does the severity of deformity influence operative strategy?
In patients presenting with an otherwise stable foot who have excessive soft tissue breakdown from bony prominences, exostectomy can be effective.48,49 While exostectomy has been reported to be effective with healing rates as high as 75%, a recent study cautioned against exostectomy confined to the lateral column, suggesting that it may increase the need for revision surgery because of calcaneal inclination change.49 Likewise, in patients with severe equinus and a stable foot, Achilles tendon lengthening (ATL) has been effective, and a study by Tiruveedhula et al. found that ATL followed by weight-bearing TCC slowed and, in some cases, reduced midfoot CN.50
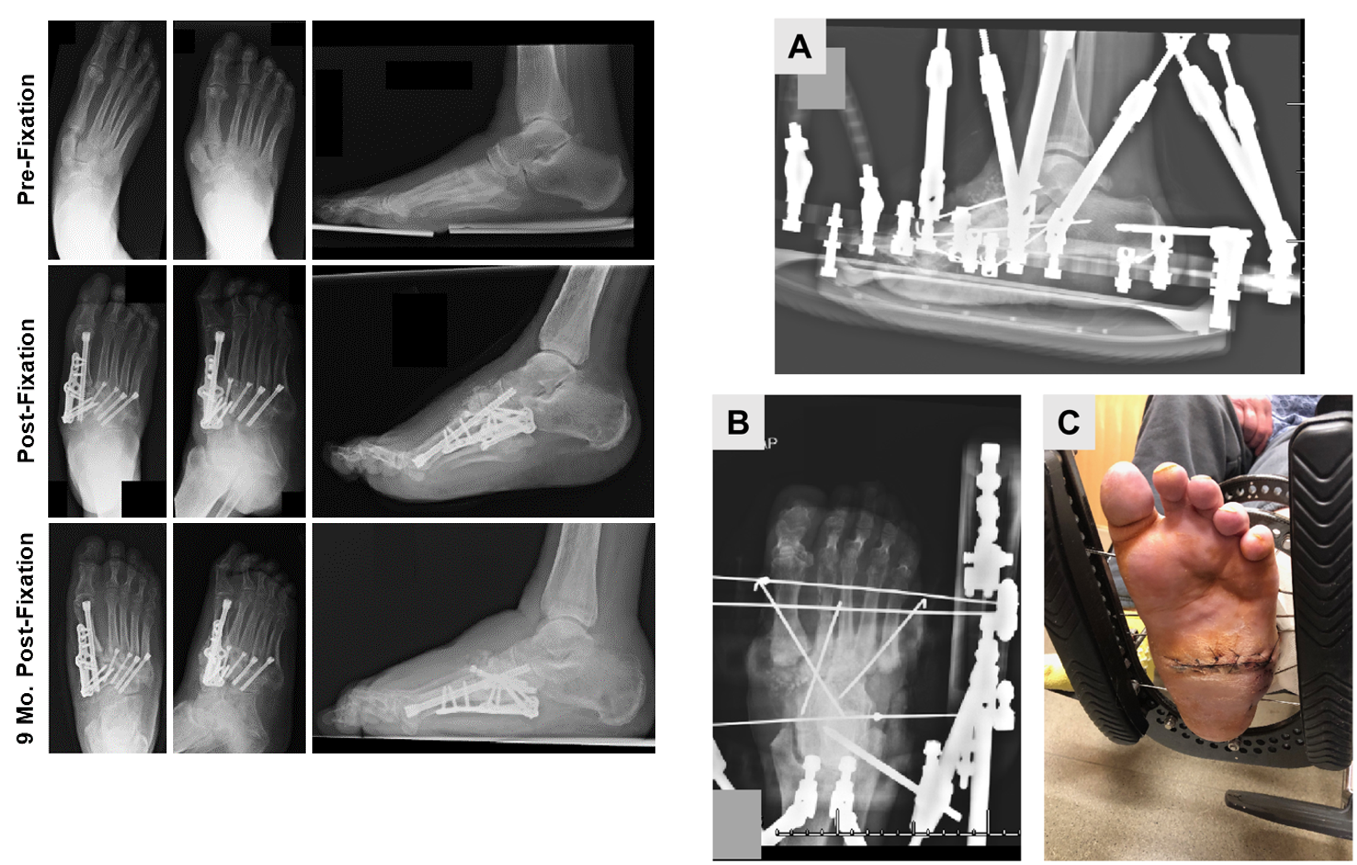
For patients with severe deformities not amenable to bracing, reconstruction can be achieved through arthrodesis using internal fixation osteotomies, external fixation, or a combination of both [Figure 3]. Multiple options exist for achieving a sound arthrodesis, including Kirschner wires, screws, plates, IM nails, beaming, and a superconstruct method.

Recently, an IM nail for hindfoot and ankle CN is a popular method. Moonot et al. reported that tibiotalocalcaneal nailing can effectively achieve a sound arthrodesis, even in patients presenting with severe loss of the talus.51 Furthermore, a prospective cohort study of 61 patients treated with tibiotalocalcaneal arthrodesis with a retrograde IM nail reported only two cases of nonunion, improved American Orthopaedic Foot and Ankle Society (AOFAS)-hindfoot scores, and reduced pain.52 Other authors have evaluated using an IM nail with an internal pseudoelastic nitinol compression element during tibiotalocalcaneal arthrodesis and reported a CT-based tibiotalar union of 71% in CN patients.53 In addition to the IM nail, Pradana et al. recently demonstrated improvement in AOFAS-hindfoot scores by performing ankle arthrodesis using a double posterior lateral plating approach.54
Beaming is another popular method of correcting midfoot CN deformity, and a recent biomechanical study found it to provide a more robust construct when compared to plantar plating.55 A case series by Santos-Vaquinhas et al. reported that 80% of patients treated with midfoot fusion with an IM beam and a lateral column bolt were ulcer-free and obtained a plantigrade foot. However, their work also reported high failure rates with complication and reoperation rates of 80% and 40%, respectively.56 Another study also reported an ulcer-free stable plantigrade foot in 84% of patients that underwent midfoot reconstruction with IM beaming, as well as improvements in Meary’s angle and a 46% rate of midfoot union on final imaging.57 Although, much like the aforementioned case study, high rates of complications, including deep infection and progression to amputation, were noted.57
The superconstruct technique has improved internal fixation by extending the IM beam into the unaffected joints. Recently, Manchanda et al. evaluated if the inclusion of the subtalar joint in the arthrodesis would be beneficial and reported a reduction in the odds of complication when subtalar arthrodesis was included during the reconstruction. Furthermore, they reported a negative correlation between the number of screws being used and the complication rate, suggesting that more hardware may be beneficial.58
One of the challenges associated with using the IM fusion bolts during stabilization of the medial column is their propensity to loosen and disrupt a sound reconstruction.59 Consequently, Melhorn et al. evaluated a high-profile threaded fusion bolt (HTFB). They found patients treated with an HTFB had higher rates of bony consolidation after three months and improvements in Meary’s angle after one year.60
Another difficult decision when performing internal fixation is figuring out what to do about the lateral column. Prior literature has suggested avoiding fusion of the lateral column during internal fixation to preserve the foot biomechanics. Interestingly, Derner et al. reported that lateral column arthrodesis in a non-neuropathic patient can provide pain relief and high rates of patient satisfaction, as well as low rates of revision in patients with post-traumatic degenerative joint disease and those with CN.61
Peritalar complex CN is exceptionally challenging and carries a high risk of amputation.62 El-Mowafi et al. reported improved mean AOFAS scores and bony fusion in 29 of 38 feet using a combination of Ilizarov external fixation and plates and locked nails for internal fixation.62 As such, a combined approach for patients with peritalar complex CN may be a viable option.
Over the last several years, external fixation has become a popular method because of its ability to be used in patients with active infection.44 In 2021, Wirth et al. demonstrated its effectiveness for limb salvage, with the latter utilizing an Ilizarov fixator and finding positive results even in chronic osteomyelitis.7 Moreover, closed arthrodesis with an Ilizarov ring external fixator is affordable compared to open approaches.63
A recent 7-14-year follow-up of 10 CN patients who presented with active ulceration and infection were treated with a Taylor Spatial Frame, which reported nine patients (9/10, 90%) were infection-free, ulcer free, and had a stable plantigrade foot amenable to diabetic footwear.64 Additionally, El-Mowafi et al. reported high rates of clinical and radiographic union in patients that underwent a combination of retrograde IM nail and circular external fixation, leading to improvement in AOFAS scores for all 24 patients.6
While many have successfully used internal fixation, external fixation, or a combination of both, research has not found one method superior.65 Yammine et al. performed a large meta-analysis to compare IM nailing with external fixation. It concluded that IM nailing is better suited for patients with ulcers along the medial or lateral aspects of the sole or in patients who lacked ulceration altogether. In contrast, external fixation benefits patients with plantar ulcers to avoid the plantar approach for nail insertion.8 Dayton et al. compared internal and external fixation complications and found that the odds of a successful outcome with internal fixation were 0.52 times greater than with external fixation.66 Other approaches that have been proposed are the combined use of interlocked IM nails with ring external fixation and a midfoot wedge resection using a plantar approach to correct the rocker bottom deformity.67,68
What operative adjuvants are being used?
Several operative adjuvants can help improve patient outcomes. Niazi et al. demonstrated in a sample of 70 patients, of which nine were identified to have CN that the use of an adjuvant antibiotic-loaded absorbable bio-composite could help achieve cure rates in up to 90% of patients with concomitant foot ulcers and osteomyelitis.69 Loveland et al. performed a retrospective multicenter case series examining the use of rhPDGF-BB/β-TCP graft to prevent nonunion in patients with CN that underwent joint fusion and found that the mean time to fusion is 13.09 ± 4.87 weeks. Only six patients were reported to have developed nonunion.70
COMPLICATIONS
The main complications that occur with nonoperative management are related to skin breakdown. At the same time, postoperative infection, re-ulceration, nonunion, hardware failure, and regaining the ability to walk are the main concerns following reconstruction procedures. Some research has estimated the 3-year mortality rate as 10.6%.71 A 2022 retrospective study found that 38.7% of patients developed a new infection, 41.9% had new ulcers, and 19.4% went on to require a below-the-knee amputation, which carries its complications of phantom pain, difficulty with prosthesis fitting due to fluid shifts, and inability to ambulate without a prosthesis.72 Sohn et al. described that CN alone does not pose an increased risk for amputation, but the risk is 12 times greater when a patient has ulceration.73
Anatomical location plays a role in outcomes and complication rates. In terms of functional recovery, patients who undergo ankle reconstructions have been found to have a 70% lower chance of returning to walking than patients who undergo reconstructions of the medial column. Patients are also 3.3 times as likely to undergo amputation compared to patients with reconstructions in the midfoot.71 Additionally, another study that evaluated 223 feet that underwent operative correction reported that 7 patients died within a year of surgery, 15 underwent amputation, and of these patients, they found that those with a dislocation pattern or varus deformity were the least likely to achieve a favorable outcome.74 Furthermore, Waibel et al. found an association between patients presenting with midfoot CN and the development of contralateral ulcers, suggesting the contralateral limb must be monitored.75
CONCLUSION AND AUTHORS’ PREFERRED METHOD OF TREATMENT
Managing Charcot patients in our practice is dictated initially by staging and the presence of an ulcer and underlying infection. Based on our institution’s pathologic staging research and cost-effective research data, we favor mid-tibia amputation for patients at high risk of complications from limb salvage surgery and who are also at high risk for failing limb salvage. In those without an ulcer, we begin with TCC to achieve a braceable, infection-free, plantigrade foot. The timing of surgery and method of internal fixation is highly dependent on host factors and is tailored individually to each patient. Patients who would benefit from reconstruction but are more likely to fail casting are taken to the operating room early, regardless of clinical stage. Those with an ulcer but less likely to undergo amputation undergo a staged reconstruction with debridement, Ilizarov frame application, and deformity correction with staged reconstruction once the ulcer is closed and the patient is clear of infection before implanting hardware. Lastly, a multidisciplinary approach, including infectious disease specialists in the clinic, a therapist trained at TCC, and medical doctors skilled at glycemic control, is essential for achieving paramount success in treating Charcot. Hopefully, as clinical research becomes more available, we can use best practice guidelines to tailor our approach more systematically, which is most effective for patients and our health system.
DECLARATION OF CONFLICT OF INTEREST
Michael Aynardi reports consulting fees from Zimmer Biomet, Stryker, and Arthrex. Michael Aynardi has also received research support from Arthrex unrelated to this manuscript.
All other authors do not have any potential conflicts of interest related to the content presented in this manuscript.
DECLARATION OF FUNDING
The authors received NO financial support for this manuscript’s preparation, research, authorship, and publication.
DECLARATION OF ETHICAL APPROVAL
Institutional Review Board approval was not required for the production of this manuscript.
DECLARATION OF INFORMED CONSENT
No information (names, initials, hospital identification numbers, or photographs/images) in the submitted manuscript can be used to identify any patients.
ACKNOWLEDGEMENT
We would like to thank the following individuals for their expertise and assistance throughout all aspects of our study and for their help in writing the manuscript: Vincenzo Bonaddio MD and Zachary Koroneos.