
Introduction
The Lisfranc joint complex, or tarsometatarsal joint (TMT) complex, is essential for maintaining midfoot structure and stability. Lisfranc injuries represent a multifarious group of injuries that can be categorized on a spectrum based on the disruption of ligamentous structures, osseous structures, or both. They can range in severity from high-energy injuries with severe disruption of the bony architecture to low-energy ligamentous strains, tears, or joint dislocation.1,2 Notably, purely ligamentous injuries have shown inferior outcomes with open reduction and internal fixation (ORIF),3 making these injuries devastating and challenging to treat. While Lisfranc injuries account for a relatively small percentage of foot injuries, affecting only 1 in every 55,000 individuals in the United States,4 these injuries can lead to progressive complications if midfoot stability is not achieved, often leading to high rates of disability due to arch collapse, gait abnormalities, difficulty in returning to sport or work, chronic pain, and posttraumatic arthritis.3
Operative management includes ORIF or primary arthrodesis. To date, various options of ORIF exist, including transarticular screws, dorsal-bridge plating, and more recently, flexible fixation methods including a suture Endobutton, Tightrope, and InternalBrace (Arthrex Inc, Naples, FL).4–7 Flexible fixation techniques have been studied as a potential alternative for patients with Lisfranc injuries to obviate the need for hardware removal. These techniques have been shown to decrease post-surgical joint immobilization and minimize articular cartilage damage seen with transarticular screws while allowing for physiologic motion across the Lisfranc joint complex.1,7,8
The Arthrex InternalBrace Lisfranc fixation repair (Arthrex, Naples, FL) system is a novel flexible fixation surgical technique used to repair Lisfranc ligament injuries and is indicated for both acute and chronic injuries.7 It offers potential advantages to other ORIF techniques, including avoidance of a second procedure for device removal, collagen ingrowth, reduced iatrogenic cartilage damage, and avoidance of irritation to the tibialis anterior tendon.7,9 A recent biomechanical study found the InternalBrace to be comparable in stability to transarticular crossed screws.10 Albeit, since it was approved by the Food and Drug Administration (FDA) in 2019, there are no clinical data reported for patients who underwent ORIF with this device.4,5,7
Therefore, the present study aimed to evaluate early postoperative outcomes in patients who underwent ORIF with the InternalBrace. We sought to explore patient demographics, time to return to work/sport, and determine postoperative complications in patients treated with this device.
Methods
Data Collection
This study received Institutional Review Board approval (IRB), and all methods were carried out with respect to relevant guidelines. A retrospective case series was performed on patients with isolated ligamentous Lisfranc injuries who underwent ORIF with the InternalBrace between October 2019 and August 2021. A single, board-certified, fellowship-trained orthopedic surgeon performed all surgeries. Both male and female patients aged 18 to 58 were included with an interosseus and/or ligamentous Lisfranc injury diagnosed via preoperative radiographs and computed tomography (CT) imaging. No patients were excluded from the study.
Procedure
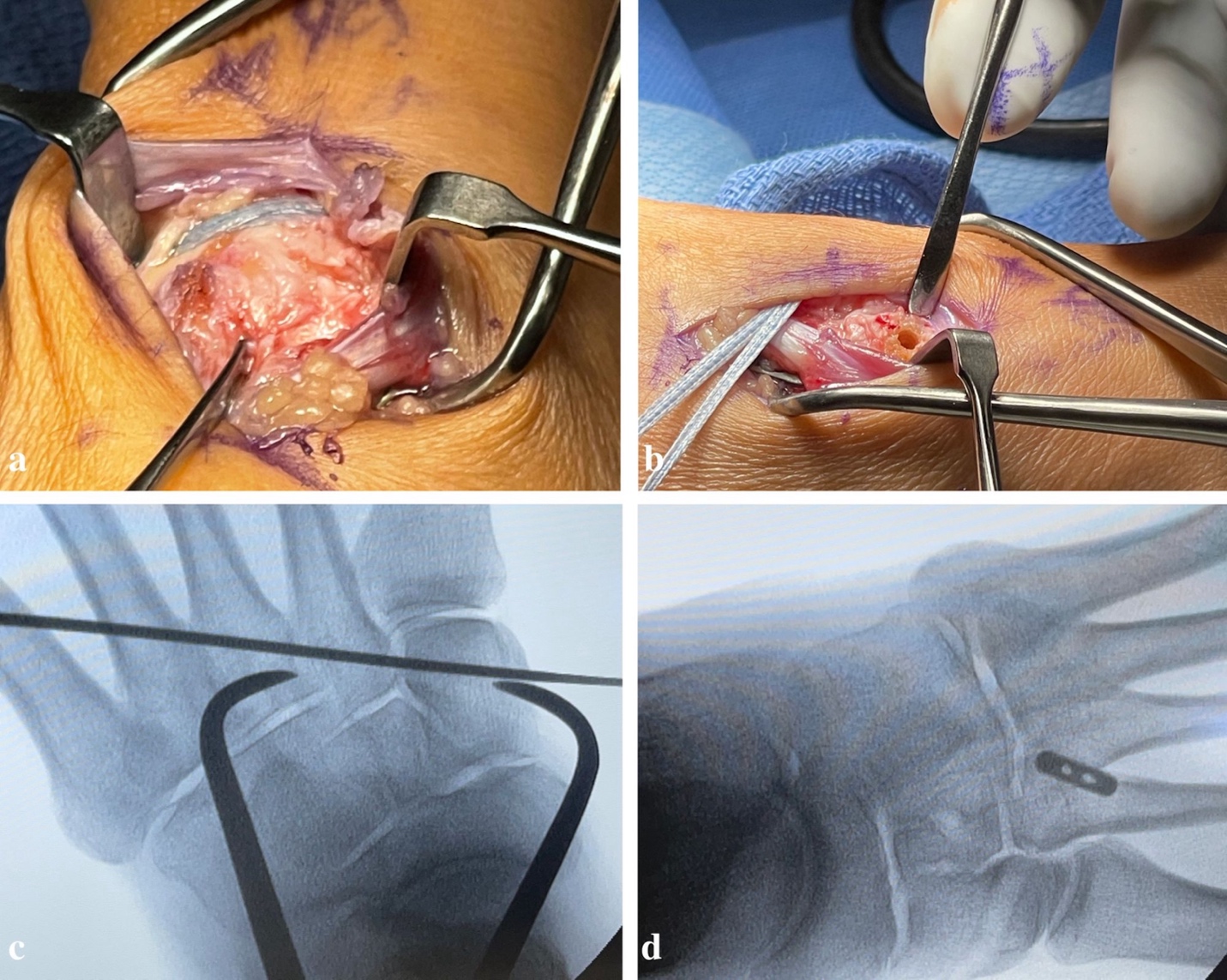
This procedure was indicated in patients with isolated ligamentous Lisfranc injuries only. Operative treatment was performed under general anesthesia with a regional block. A dorsal incision was utilized for exposure and reduction via three separate windows: a medial window to evaluate the Lisfranc articulation with the intercuneiform, another window for vessel dissection and protection, and a lateral window for exposure of the lateral aspect of the second metatarsal base for hardware implantation. Stress examination and a Freer elevator “drive-through” sign were performed to confirm a Lisfranc ligament tear and evaluate for subtle disruption of intercuneiform joints when present. Before reduction, bony surfaces of the Lisfranc interval and intercuneiform space were debrided of fibrous tissue with curette and rongeur. Fixation consisted of placing a Weber clamp on the base of the second metatarsal and medial cuneiform through two small incisions, medial and dorsolateral. Next, a guidewire is placed along the planned fixation trajectory from the lateral base of the second metatarsal to the medial cuneiform. A collagen-coated 2 mm suture button and tape were passed from lateral to medial, with the button flush against the second metatarsal cortex. A 4.75 mm SwiveLock anchor was then placed in the medial cuneiform to hold the Lisfranc interval reduced after predrilling and tapping. Next, a 3.4 mm drill bit was used to drill the central portion of the middle cuneiform. The suture tape limbs were passed deep to the tibialis anterior tendon and associated neurovascular bundle, directing them towards the middle cuneiform. The suture limbs were then threaded through the 3.5 mm interference anchor placed on the middle cuneiform and securely positioned, ensuring proper fixation of the supplemental limb [Figure 1].

Post-Operative Care
Following surgical treatment, patients were splinted for two weeks and made touchdown weight-bearing on crutches. Patients were permitted to have their foot in contact with the ground with enough weight for balance, 20lb maximum, and instructed not to push off with their foot. This protocol was not changed based on the weight of the patient. Sutures were removed at two weeks, and Steri-Strips were placed over the incision. Patients were then transitioned to a CAM boot and instructed to perform deep knee bends using a counter or chair for balance while progressing twenty pounds per week until they could weight-bear as tolerated. At six weeks post-operatively, standing radiographs were reviewed, and patients were instructed to begin full weight-bearing as tolerated in a CAM walking boot with a gradual transition to normal shoe wear over the next six weeks.
Twelve-week postoperative radiographs assessed alignment and were evaluated for any widening at the Lisfranc joint. Patients could typically return to work/play as tolerated at this time.
Outcomes
The primary endpoints of this study were time to weight-bearing as tolerated and unrestricted return to work or sport. This was evaluated in patient charts by identifying a clinic note stating that the patient returned to weight bearing or activity without restriction. Patients were evaluated at 2- weeks, 6- weeks, and 12- weeks following surgery. At the 2-week follow-up appointment, patients were evaluated in the clinic for complications (i.e., infection, hypersensitivity, and paresthesia). Radiographs were obtained at both 6- and 12 weeks following surgery. Radiographs were evaluated for hardware complications and disuse osteopenia surrounding the tarsometatarsal joint [Figure 2]. Patients were then subsequently seen in the clinic at six months post-op.
_injur.png)
Results
From October 2019 to August 2021, nine patients underwent ORIF with the InternalBrace, including four females and five males. The mean age of participants was 29 (standard deviation (SD) 16; range 18-58). The majority of patients (n=7) were white and non-Hispanic. Only one patient was a smoker. Indications for InternalBrace repair included five ligamentous only and four ligamentous injuries with intercuneiform instability [Table 1]. The average follow-up time was 6.6 months (SD = 5.1). Injury type included purely ligamentous injury (n=5) and ligamentous injury compounded with intercuneiform instability (n=4). The mechanism of injury for these patients was trauma (n=3), inversions (n=4), and cutting maneuvers (n=2). All three traumatic injuries resulted from direct force events involving a crushing mechanism. These incidents included two direct impact injuries from stepping onto the dorsum of the foot during a collegiate football game and one injury from dropping a weight onto the dorsum of the foot.
The average time to weight-bearing as tolerated and unrestricted work or sport were 6.8 and 13 weeks, respectively. At the 2-week clinical evaluation, one patient experienced a complication characterized as a transient episode of hypersensitivity, which was subsequently resolved by week 12. Expected disuse osteopenia from initial immobilization was observed in five patients at the 6-week radiograph; however, this was resolved in all but one patient by the 12-week radiographs. No hardware complications were noted in all nine patients during both the 6-week and 12-week radiographic assessments [Table 1].
Discussion
Surgical treatment options for Lisfranc injuries include open reduction and internal fixation (ORIF) and primary arthrodesis. There are currently numerous options for ORIF of Lisfranc injuries, including K-wires, transarticular screws, fibertape suture anchors, and dorsal plates.4,5 More recently, there has been increasing interest in flexible fixation methods such as suture Endobutton, Tightrope, and InternalBrace. While both the Tightrope device and the suture Endobutton technique have shown good short-term results through reported case series,6,11 there is no published patient outcome data after using the InternalBrace. Our study demonstrates that the InternalBrace system can reliably be used as a flexible fixation technique in patients with Lisfranc injuries.
While proper anatomic reduction remains the key to a successful outcome of ORIF utilizing any fixation method,1,4,8 the operative treatment approach to achieve this goal remains controversial. Non-rigid fixation techniques offer advantages compared to rigid fixation with transarticular screws, such as avoidance of screw breakage and the need for later hardware removal, as well as reduction of iatrogenic damage to articular cartilage.6–8 Advantages specific to the InternalBrace include collagen ingrowth using the collagen-coated fibertape suture, obviating the need for hardware removal, and the potential for physiologic motion across the joint, as demonstrated in previous biomechanical studies.7,12,13 Additionally, by using a button that lays flush against the 2nd metatarsal, an interference screw buried flush into bone, there is a decreased likelihood of irritation of the tibialis anterior tendon.7 In a biomechanical model comparing screw, suture button, and InternalBrace, Hopkins et al. demonstrated comparable mechanical properties between the InternalBrace and suture button.9 These findings and the clinical outcomes reported in the present study demonstrate that the InternalBrace can be a successful flexible fixation option for patients with Lisfranc injuries.
Currently, there is a large discrepancy in reported Lisfranc outcomes regarding RR (return rate) and RTS/P (return to sport/play) due to the differences in the mechanism of injury, anatomy of injury, and management (operative vs. non-operative). Few meta-analyses compare the operative management options within the different types of Lisfranc injuries due to the large heterogeneity in databases and case series.
Regarding low-energy Lisfranc injuries, i.e., most athletic activities, current meta-analyses suggest a discrepancy in the RTS/P when comparing primary arthrodesis (PA), primary partial arthrodesis (PPA), and ORIF, with some studies showing an advantage in primary arthrodesis compared to ORIF.14–17 One large meta-analysis investigated return to sport in operatively managed Lisfranc injuries and demonstrated an RTS of 19.6 weeks and 22.0 weeks in ORIF and PPA, respectively.15 While limited due to sample size, their return to play and work averages are comparable to that of the time to unrestricted weight bearing demonstrated by the InternalBrace at 13.2 weeks (12.1-18.0)
While there are currently no case series or meta-analyses analyzing the Internal Brace, other flexible fixation techniques in Lisfranc injuries have been studied. Case series regarding the tightrope have shown the safety of the device and return to activity within six months of surgery, as well as stability of the joint as measured through joint diastasis and reduction in American Orthopaedic Foot and Ankle Society (AOFAS) pain scores.6,18 One case series regarding high-level athletes with Lisfranc injuries failing conservative measurement demonstrated a similar return to play time of fewer than six months while increasing AOFAS function scores.19 Overall, these small case series demonstrate the safety of flexible fixation and the need for further randomized control trial studies and meta-analyses.
In their 2020 biomechanical study, Hopkins et al. studied the mechanical properties of InternalBrace in the treatment of Lisfranc injuries in a sawbone model parametrically to suture button and screw fixation in an effort to determine if the mechanical properties of InternalBrace could theoretically support early weight-bearing by tolerating a full- weight-bearing load.9 Though obviously limited by utilizing a sawbone model, these authors report that InternalBrace shows properties that appear comparable to the suture button while being less rigid than the screw in load to failure. In their appraisal of the data, these authors submit that during cyclical loading, the InternalBrace showed properties appropriate for anatomic fixation with protected weight bearing. However, it has increased failure rates with increased load and may not necessarily support early weight bearing as an independent construct.
This study is not without limitations. First and most importantly, a small sample size is reported; therefore, the conclusions should be interpreted cautiously. Second, this study was retrospective, making it susceptible to bias because of the need to rely on accurate electronic medical record documentation. Third, while we found no surgical or hardware complications, no scoring system was used to report on patient outcomes. Fourth, while our patients returned to work/sport in a time frame comparable with other ORIF methods, we could not determine what type of work or sport they were returning to. Finally, while flexible fixation techniques prevent the need for additional surgery, we did not consider the cost of the implant.
Nevertheless, despite these limitations, this study presents important clinical information regarding a novel orthopaedic implant that can help inform orthopaedic surgeons when deciding on which flexible fixation option they may use for Lisfranc injuries. Further studies are needed with large sample sizes, a more robust scoring system to evaluate outcomes, and a cost analysis to help better determine the efficacy of this implant.
Conclusions
In this retrospective case series, we evaluated the early postoperative outcomes of patients with ligamentous Lisfranc injuries treated with the Arthrex InternalBrace, a novel orthopaedic implant. We observed no early postoperative complications, and patients achieved a time to return to work or sport comparable to other methods of flexible ORIF reported. The advantages of the InternalBrace, such as collagen ingrowth, avoidance of hardware removal, reduce iatrogenic cartilage damage, and the potential for physiologic joint motion, make it a compelling option for orthopaedic surgeons. Our study supports the feasibility of the InternalBrace as a flexible fixation method for Lisfranc injuries.
The clinical insights provided by this study can help inform orthopaedic surgeons when deciding which flexible fixation option they may use for Lisfranc injuries. Further studies are needed with large sample sizes, a more robust scoring system to evaluate outcomes, and a cost analysis to help better determine the efficacy of this implant.
DECLARATION OF CONFLICT OF INTEREST
Author Michael C Aynardi participates as a consultant for Arthrex, Stryker, and Zimmer Biomet. Author Michael C Aynardi is also a member of the AOFAS vice-chair practice manager and research committee. Otherwise, all other authors declare no conflict of interest.
DECLARATION OF FUNDING
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
DECLARATION OF ETHICAL APPROVAL FOR STUDY
The Pennsylvania State University Institutional Review Board approved this study. Study ID: STUDY00006237.
DECLARATION OF INFORMED CONSENT
There is no information (names, initial, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.