INTRODUCTION
Peripheral nerve wraps following primary nerve repair or chronic nerve compression aim to decrease scar formation, improve nerve gliding, and minimize axonal escape.1–3 Multiple nerve wraps include vein wrapping, adipofascial or muscle flaps, bovine collagen wraps, porcine small intestine submucosal wraps, human umbilical cord membranes, and synthetic collagen products.2–16 The ideal nerve wrap would illicit minimal inflammatory reaction, allow nutrient diffusion without axonal escape, avoid scar-induced nerve ischemia, and promote nerve gliding without any donor site morbidity and with minimal cost.3
One commercially available nerve wrap is the AxoGuard™ (Axogen, Alachua, USA) porcine extracellular matrix (PEM) nerve wrap, which is derived from small intestine submucosal and composed of collagen fibronectin, growth factors, glycosaminoglycans, proteoglycans, and glycoproteins. It is indicated for use in peripheral nerve injuries without a nerve gap.2,17 Animal models of nerve laceration repaired with primary epineural coaptation augmented by PEM nerve wrapping have shown reduced short-term scar deposition at coaptation sites without long-term functional differences.14,18 Cadaver studies have also demonstrated improved primary epineural repair strength when augmented by PEM nerve wrap.19 Case series have also shown the use of PEM nerve wrapping in the setting of revision carpal tunnel decompression and revision cubital tunnel decompression.20,21
No consensus exists on the indications for using the PEM nerve wrap. The primary purpose of this study is to assess the operative indications for using the PEM nerve wrap by hand and upper extremity surgeons to understand better how nerve wraps are utilized.
METHODS
With institutional review board approval, all patients that received the AxoGuard™ PEM nerve wrap between February 2016 through March 2023 at a single orthopaedic practice were identified by implant records. Patients were excluded if the procedure was not conducted on the hand or upper extremity, was not performed by a hand surgery fellowship-trained orthopaedic surgeon, or if patient records did not clearly state the application of the nerve wrap. A retrospective review of the patient’s electronic medical record was performed. Patient demographics, pre-operative exam, and testing, history of present illness, intra-operative findings, and complications were recorded. The decision to utilize the PEM nerve wrap was made by the operative surgeon at the time of the procedure based on intra-operative findings.
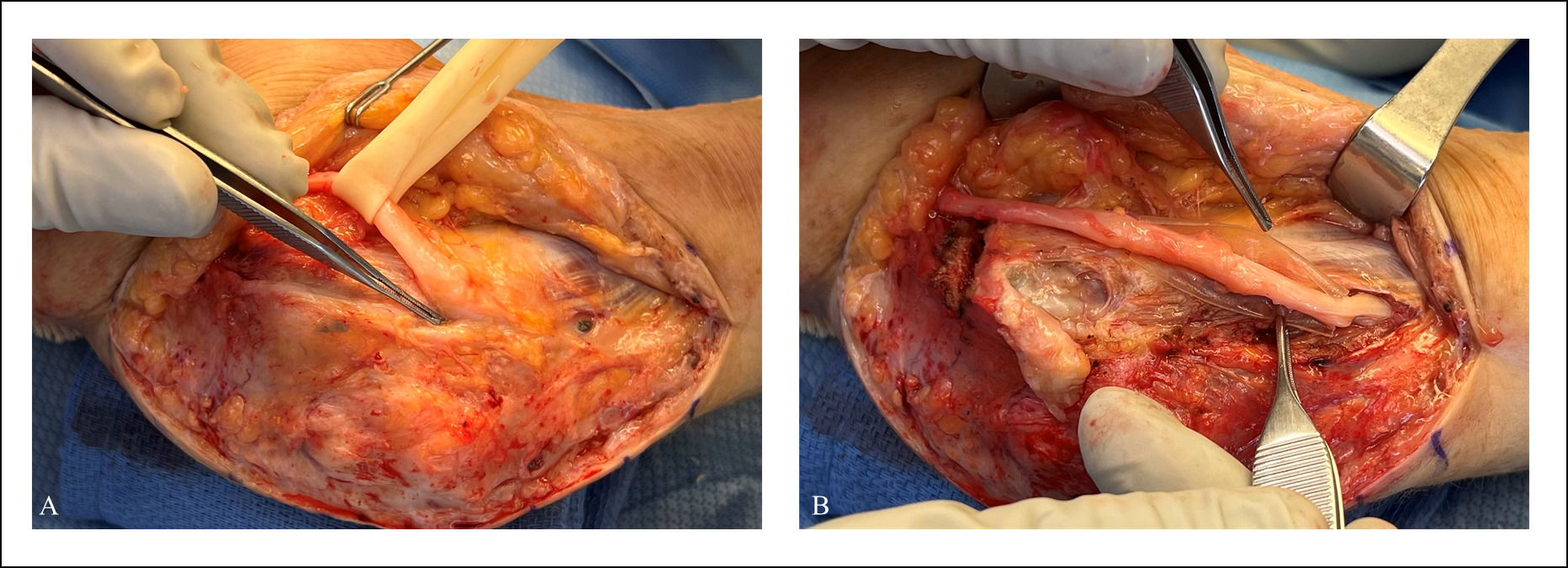
Patients were categorized based on the clinical indication for nerve wrap use into three groups: Acute, Chronic, and Other. Patients in the “Acute” group presented with acute nerve injuries, such as blunt trauma, fracture, laceration, or iatrogenic injury attributed to the onset of symptoms. Patients in the “Chronic” group presented with signs and symptoms of chronic nerve compression undergoing decompression without a history of traumatic or iatrogenic nerve injury preceding symptom onset [Figure 1]. Patients in the “Other” group underwent nerve wrapping following mass excision and joint contracture release procedures.

Continuous data were presented as a median followed by the first quartile (Q1) and third quartile (Q3). Categorical data were presented as a cell count (percent of total count).
RESULTS
Overall, implant records identified the PEM nerve wrap was utilized in 147 procedures during the study period. Of these, 29 procedures were excluded because operative records did not confirm using the nerve wrap, and 14 were excluded because surgery was performed on the lower extremity. This resulted in a final study group of 104 procedures (of the initial 147, 71%) performed on 102 patients by 13 orthopaedic hand and upper extremity surgeons. The average time from procedure until data collection was 3.5 years (range 0.5 to 7.5 years). Two patients underwent bilateral carpal tunnel revisions. Patient demographics are presented in [Table 1]. The indication for surgery was acute traumatic injury in 57 patients (55%), chronic nerve compression in 41 patients (39%), and six patients (5.8%) underwent either mass removal or joint contracture release involving neurolysis [Figure 1]. The nerve that underwent nerve wrapping in our cohort is summarized in [Table 2].
Among the patients with acute nerve injury, 43 (75%) had an acute laceration to the hand and upper extremity. The remaining 14 (25%) had an alternative acute nerve injury: eight fractures, two iatrogenic post-op nerve deficits (one acute radial nerve palsy following long stem reverse total shoulder arthroplasty and one emergent paresthesia after first dorsal compartment release), two gunshot wounds, one blunt trauma without fracture, and one patient with persistent paresthesias following blood draw. Symptoms were present for a median of 15 days (Q1 8 days, Q3 54 days) pre-operatively. Nine patients (16%) had a pre-op EMG, of which seven were consistent with nerve injury, one was normal, and one demonstrated early complex regional pain syndrome. Pre-operative sensory and motor symptoms were present in 98% and 49% of patients, respectively. Intraoperative description of the nerve was available for 86% (49) of patients. Of these, complete nerve laceration was noted in 10 patients (20.%), and partial nerve lacerations were noted in 17 patients (35%). The remaining patients had intact nerves but were noted to have neural inflammation in 13 patients (27%) and scarring or perineural fibrosis in seven patients (14%). Two patients (4.1%) had normal-appearing nerves intra-operatively for exploration after acute post-operative nerve deficits. Nerves were repaired in 44% of patients (24 primarily with sutures and one with nerve conduit). The remaining patients underwent neurolysis without repair.
Among the patients with chronic nerve compression, patients experienced symptoms for a median of 571 days (Q1 297 days, Q3 1,313 days). Ninety-five percent of these patients (39/41 patients) underwent pre-op EMG, which was consistent with nerve compression in 35 patients. Two patients’ EMGs were interpreted as normal, and two EMGs demonstrated cervical radiculopathy. All (41/41) patients had pre-op numbness and tingling, but only 51% (21/41 patients) had pre-op weakness. Revision carpal tunnel and revision cubital tunnel were performed on 26 (63%) and nine (22%) patients, respectively. The remaining six patients underwent nerve decompression following remote injury or remote surgery in the local environment of the nerve: two patients with prior elbow blunt trauma, one patient with total elbow arthroplasty, one patient with non-operative distal radius fracture, one patient with retained glass foreign body from 32 years prior, and one patient with a history of forearm laceration four years earlier. In all cases, the nerve was in continuity but had significant scarring, adhesions, and/or nerve inflammation for which external neurolysis and nerve wrapping were indicated.
Among the other six patients, the indication for nerve wrapping was mass removal with nerve dissection in five patients, and one patient underwent nerve wrapping following proximal interphalangeal joint contracture release.
Three patients (2.9%) required reoperation, two in the acute group and one in the chronic group. [Table 3] describes these complications in detail but generally consist of persistent or recurrent nerve paresthesias following nerve wrapping re-operation. There were no cases of nerve wrap rejection, extrusion, or infection.
DISCUSSION
This case series summarizes the indications for using PEM nerve wrap by 13 orthopaedic hand and upper extremity surgeons at a single orthopaedic surgical practice. Over half of the patients underwent PEM nerve wrapping after an acute injury for which nerve exploration was indicated, the majority of which occurred after a hand or forearm laceration. Just under half of these patients underwent primary epineural nerve repair (44%). Epineural nerve repair is the gold standard treatment for peripheral nerve injuries without a gap.22 In nerve recovery, animal studies have demonstrated that scar formation at the repair site is associated with smaller compound action potentials and slower conduction velocities23 Nerve wraps have been developed for use in peripheral nerve injury to create a local environment that limits intraneural scarring and axonal escape and promotes nerve gliding.14 Although animal studies have shown decreased fibrosis at the repair site in the short term with PEM nerve wrapping, they have not shown any difference in functional outcomes at the final follow-up interval.14,18 Here, we demonstrate the use of the PEM nerve wrapping in the setting of acute upper extremity peripheral nerve injury, both as an adjunct to primary repair and as an adjunct to external neurolysis in the setting of neural contusions and perineural fibrosis. To determine any difference in treatment outcomes, further studies must compare PEM nerve wrapping to conventional repair without nerve wrapping.
The second most common indication for PEM nerve wrapping was chronic peripheral nerve compression, most commonly in patients presenting with recurrent carpal tunnel or recurrent cubital tunnel after prior release with intra-operative epineural fibrosis and scarring. Recurrent carpal tunnel and cubital tunnel are attributed to recurrent compression, incomplete release, or perineural scarring.24 Recent reports by Imran et al.20 and Papatheodorou et al.21 have reported positive post-operative outcomes for their patients, each undergoing revision carpal and cubital tunnel with external neurolysis and PEM nerve wrapping, respectively. Alternative nerve wraps have also been reported in the management of revision carpal and cubital tunnel syndrome, including collagen nerve wrap and autologous fat pad transfer9,13,24–26 In this retrospective analysis, the use of PEM nerve wrapping in revision carpal and cubital tunnel syndrome was also a common indication in 26 and nine patients, respectively. All these patients had a clinical history and physical exam consistent with recurrent nerve compression, and nerve compression was confirmed on electrodiagnostic testing in 89% (31/35 patients). Two patients had a normal EMG but a high clinical suspicion for recurrent compression, and two patients did not undergo pre-op EMG testing.
PEM nerve wrapping was also indicated for six patients with chronic compression in the setting of remote traumatic injury or remote surgery in the compressed nerve’s local environment. Similarly, five patients had PEM nerve wrapping at the time of mass excision, and one had PEM nerve wrapping at the time of finger contracture release. In each of these procedures, PEM nerve wrapping was indicated by the operative surgeon to minimize perineural scarring in the setting of a poor local environment that the surgeon thought would predispose to increased perineural scar formation. To our knowledge, this indication has not been previously reported in the literature.
An overall reoperation rate of 2.9% was identified. Three patients experienced persistent post-operative numbness and paresthesias attributed to the injured nerve requiring revision procedures at one year, three years, and four years post-operatively, respectively, as summarized in [Table 3]. Intra-operatively, one patient had recurrent perineural scarring and adhesions, while two of these patients had developed neuromas at the repair sites. Prior reports of PEM nerve wrap for revision carpal tunnel and cubital tunnel syndrome have reported no recurrent symptoms at a follow-up of 23 months and 24 months, respectively.20,21 One case report in the literature documents a necrotic granulomatous inflammation two and a half months post-operative following PEM nerve wrapping.27 In this retrospective analysis, no complications associated with adverse reactions to the PEM nerve wrap were observed, such as rejection, infection, or extrusion.20,21
There are several limitations to this study. First, this retrospective analysis attempts to review and analyze the indications for using PEM nerve wrapping based on a chart review of continuous cases in the upper extremity with the AxoGuard™ porcine extracellular matrix (PEM) nerve wrap. However, the effect of the nerve wrap on surgical outcomes cannot be ascertained due to a lack of a control arm and the heterogeneous nature of the nerve injuries or dysfunctions. Further, we do not present an exhaustive list of reasons PEM nerve wrapping may be used, but rather a snapshot of how it has been used over five years in a single orthopaedic practice. Lastly, reoperations and complications are limited to the documentation of care provided in the available medical records. They may underrepresent complications and subsequent reoperations that these patients may have undergone if they sought care elsewhere.
CONCLUSION
In summary, in this consecutive series of 104 surgeries of the upper extremity using the AxoGuard™ PEM nerve wrap, it was found to be used in acute nerve injury cases 55% of the time and nerve decompression cases 39% of the time. Moreover, three reoperation cases were noted, but zero cases of nerve wrap infection, rejection, or extrusion. These findings are helpful because they highlight common situations in which a PEM nerve wrap may be used to augment nerve repair or nerve decompression and highlight an important area for future research. Based on the available data, the effect of PEM nerve wrapping on surgical outcomes to isolated nerve repair, neurolysis, or decompression cannot be determined. Further studies are required to determine how much PEM nerve wrapping correlates to outcomes.
Declaration of conflict of interest
One author (AMI) is a consultant for Axogen and has received research support for Axogen in the past 36 months.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
Institutional Review Board approval was received from Thomas Jefferson University.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.
Acknowledgments
None