INTRODUCTION
Closed biceps rupture usually occurs at the proximal tendon origin of the long head; less commonly it is disrupted at the distal tendon insertion.1 Only a few reports have described a midsubstance muscle belly rupture. Gilcreest first reported isolated closed rupture of the short head of the biceps brachii muscle belly in 1934 in 2 cases out of 100 biceps lesions. However, the mechanism of injury was not described.2 Levine and Heckman described a direct compression mechanism in military parachutists whereby the mid-arm was forcibly abducted and compressed against the parachute cord.3 DiChristina and Lustig reported a similar mechanism by a water skiing rope.4 Shah and Pruzansky alternatively described a compressive mechanism of the short head of the biceps against a car window frame; while riding in the passenger seat, the patient’s hand struck a car door on the street while the mid-arm struck the window frame in an abducted and externally rotated position.5 We present an additional case resulting from an automobile-compression mechanism, which produced a more global closed injury to the anterior compartment muscles of the arm.
CASE REPORT
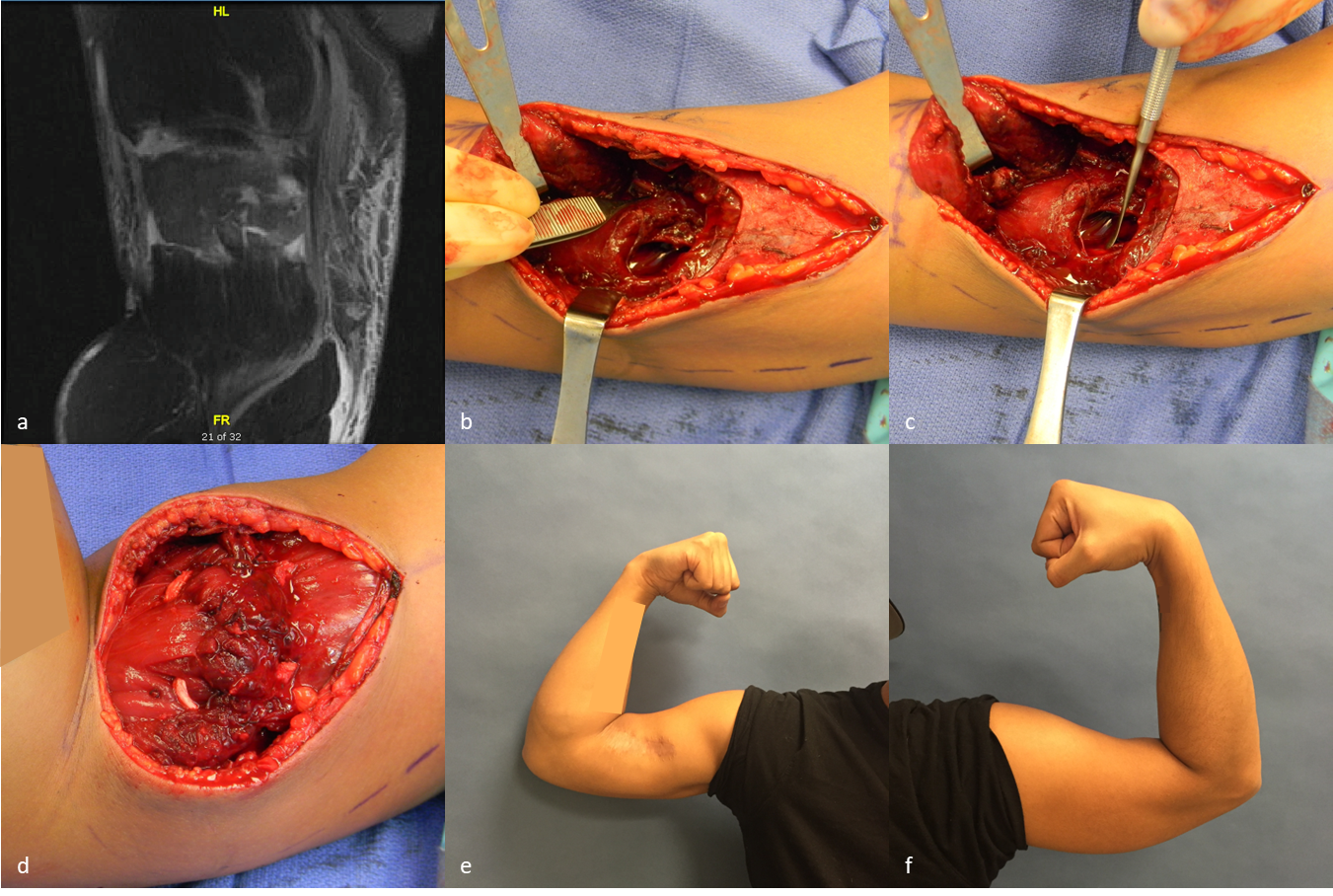
A 28-year-old right-hand-dominant male presented for a third opinion 12 days following an injury to the right arm with persistent pain and weakness. He was riding in the passenger seat of a car with his right hand outstretched in an externally rotated and abducted position out of the window to wave to another person. Another car door on the street suddenly opened and hit his hand, forcing his mid-arm into the rear part of the window frame. On examination, he had ecchymosis and a deformity of the biceps contour. He was tender at the arm mid-portion over a palpable defect in the muscle belly. Active elbow arc of motion was limited to 30-80° of flexion. Pain limited active forearm rotation, but passive forearm rotation was full. Using the Medical Research Council grading system, he had 2/5 strength of elbow flexion and supination with the elbow flexed to 90 degrees. The neurological exam was normal, including lateral antebrachial cutaneous nerve distribution. Radiographs were negative for bony injury. Magnetic resonance images (MRI) demonstrated complete mid-substance rupture of the biceps brachii muscle belly with 3 cm of retraction of the proximal stump [Figure 1A]. The MRI report also suggested a brachialis muscle belly rupture of the medial 30-50%.
_sagittal_mri_of_the_biceps_showing_the_proximal_muscle_belly_(top)_and_distal_muscle_b.png)
Operative repair of the ruptured muscles was recommended to restore anatomy and optimize patient outcomes. We approached the arm through an anterior exposure. Incision of the anterior brachial fascia revealed a large hematoma. The biceps brachii was completely ruptured at the muscle belly with a 3 cm gap; the tear morphology was such that the proximal muscle belly fit as a “shell” around the distal muscle belly. The brachialis muscle belly had a similar appearance. The lateral antebrachial cutaneous nerve, median nerve, and brachial artery were all visible in the field and noted to be in continuity [Figure 1B and 1C]. The brachialis muscle was repaired first with the elbow in 90 degrees of flexion and using an anchor suture technique described by Julien and Mudgal.6 The biceps was repaired in the same fashion and augmented with a semitendinosus and gracilis allograft measuring 4.5 mm x 240 mm and 5 mm x 240 mm, respectively [Figure 1D]. We chose to augment the repair given the delay in presentation and the poor integrity of the avulsed tissue. After repair, the elbow extended to 50 degrees short of full extension without tension. He was placed into a long arm cast for four weeks with the elbow flexed to 90 degrees and full forearm supination. After immobilization, the patient began a rehabilitation program focusing first on increasing active extension by 15-30 degrees per week, followed by a strengthening program at ten weeks. At the final visit, nine months after surgery, he reported no complaints or functional limitations; however, the overall contour of the arm was not fully restored [Figure 1E and 1F]. His active range of motion was 0-140° of flexion and 65° of supination. Isometric elbow flexion strength was assessed by a dynamometer (Computer Sports Medicine Inc., Stoughton, MA) for both peak torque (highest recording) and average torque of five repetitions with the elbow positioned at 60° and 90° flexion [Table 1].
DISCUSSION
Closed rupture of the biceps muscle belly is a rare injury; only a few heterogeneous reports in the literature provide awareness and guidance.1–5,7,8 Therefore, diagnosis can be difficult and delayed, which was the case for our patient. The optimal management plan, repair technique, and outcomes are not well known.
Surgeons may not initially diagnose muscle belly rupture. Classically, the mechanism of injury, reported in paratroopers by Heckman and Levine in 1978, described an external compression by a parachute cord as it is forcefully deployed.3 Only more recently have other mechanisms, such as forceful abduction by a water skiing rope and eccentric loading during gymnastics, been reported.4,8 Our case had a nearly identical mechanism to that in Shah and Pruzansky’s report,5 whereby the arm was forcibly abducted by the street-car door and simultaneously compressed against his own car door window frame. Most reports highlight forcible elbow extension while the biceps is pulled away from a fixed compression point in the mid-arm with the shoulder abducted, generating a sudden eccentric contractile force. Additionally, the physical exam may not be forthcoming. A palpable defect or loss of biceps contour may not be initially obvious because hematoma fills the defect, and post-traumatic swelling can confound the unsuspecting clinician. A functioning lateral antebrachial cutaneous nerve may cause the clinician to underestimate the degree of soft tissue tearing. As in our case, the nerve is often intact despite a complete muscle rupture.3,5,7 Heckman and Levine noted a delay in diagnosis of up to 4-9 months in some patients.3 MRI has only recently been cited as aiding the diagnosis.5,8 However, although we feel MRI is a useful modality, the degree of tearing and increased signal hyper-intensity of the biceps injury may obscure the accuracy of diagnosing additional muscle or nerve injuries. In our case, the extent of the brachialis tear was challenging to determine preoperatively.
Non-operative management has been reported in the earlier experiences of military centers. Heckman and Levine reported on 28 soldiers who were treated with a shoulder sling followed by physical therapy: 25 complained of weakness, 12 complained of pain, and 17 complained of unfavorable cosmesis.3 The same authors also reported on aspiration of the hematoma and casting in flexion, inspired by their intraoperative findings of an intact fascia, a reducible muscle gap with elbow flexion, and an interposed hematoma. Of the ten patients treated with early aspiration, two complained of weakness, and one complained of cosmetic appearance. They noted the average flexion strength was 77% of normal with no complications.3
Surgery has the purported advantages of improving cosmesis and strength in young, active patients. Although muscle heals by fibroblastic proliferation, surgical repair approximates the proximal and distal segments, which enhances the length-tension relationship of the muscle fibers. The optimal repair technique is not known. Reports vary in citing interrupted locking sutures such as the Kessler or Mason-Allen techniques.7,8 Occasionally, the locking sutures may still not provide sufficient tensile strength, especially if the operative treatment is delayed or the tissue has poor quality. Heckman and Levine advocated for augmentation of U-shaped flaps in the biceps fascia.3 Although laboratory data has shown the anchor suture technique to be significantly stronger than the modified Kessler technique for muscle belly repairs,9 we opted to reinforce the repair with a U-shaped tendon allograft given the delay in presentation in our patient. Whether the ultimate outcome in our patient truly benefited from such an augmentation is unclear and remains, at best, speculative.
Only the two studies on paratroopers reported functional outcomes with surgery. Heckman and Levine reported that flexion strength improved to an average of 76% of the contralateral side as opposed to 53% in the non-operative group. In their delayed surgery cohort, a few months after injury, only marginal improvement in elbow flexion strength was noted (42% preoperatively to 57% post-operatively).3 Early surgical repair may lead to improved outcomes. Kragh and Basamania reported that in their series of nine paratroopers treated operatively, supination strength improved to an average of 89% of the contralateral side (range 71-121%), as opposed to 65% in the three treated nonoperatively (range 64-67%). They also noted improved appearance and subjective outcome in the operative group.7 Our patient had a similar outcome with a full arc of motion and isometric flexion strength reaching 71% to 81% of the contralateral arm, depending upon the position. Although we cannot be certain, fibrosis, atrophy, altered vascularity, innervation, or length-tension may explain why the appearance and strength were not completely restored.
Declaration of conflict of interest
the authors have NO relevant disclosures to report.
Declaration of funding
the authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
study covered under the umbrella IRB prior to study initiation.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients or participants.