
INTRODUCTION
In 1965, Drs. Shigeo Komatsu and Susumu Tamai performed the first digital replantation ever reported when they successfully reattached the thumb of a 28-year-old laborer in Japan.1 This came only three years after Drs. Ronald Malt and Charles McKhann replanted the arm of a 12-year-old boy at the Massachusetts General Hospital.2 These sentinel events marked a time when our field would never be the same again. Upon blazing this trail for us, much has changed, or at least we like to think so. As with any novel procedure, first, we learned what we could do, then spent decades learning what we should do, namely how to set expectations for patients undergoing replantation surgery. In this review, we aim to elucidate the current state of digital replantation, specifically with respect to indications and clinical outcomes.
Indications
There is no doubt that the indications for digital replantation have narrowed over the years as we reflect on the outcomes of our patients. The shift to measuring patient-reported outcomes is no doubt a part of this. The definition of success has shifted from surgeon satisfaction with survival to objective measures and patient satisfaction with function. This trend of narrowing indications has been seen not only in the United States but in other parts of the world as well.3–6 Though we have learned much, some of the indications for digital replantation have remained unchanged.7
An amputation of the thumb, regardless of the level, is typically viewed as an absolute indication for an attempt at replantation.5,7–9 This is due to the critical function of the thumb as a post for grip and opposition. These activities make up close to half of the function of the intact human hand.7,9 The functional devastation of a lost thumb is demonstrated by the litany of procedures designed for the event that the thumb is not salvageable. Some of these procedures include metacarpal lengthening, webspace deepening, pollicization, and a free toe-to-thumb transfer. Very good outcomes have been reported in each case.9–12
Another absolute indication is the amputation of multiple digits.5,7–9 As an increasing number of digits are sacrificed, the global function of the hand precipitously declines. Thus, an attempt at replantation, even if transposing the amputated digits or using “spare parts” is warranted. In these procedures, priority is taken away from replanting the parts where they came from and given to replanting them in more functional positions for the patient.9,13–15 Quite a bit of success has been reported with both techniques, providing the patient with better function compared with revision amputation alone.
The final absolute indication for digital replantation is an amputation in a pediatric patient.7,8,16 With children having a longer life expectancy than adults and given their superior biology for healing compared to adults, the indications to perform a replant in a child are typically much more aggressive.7,16
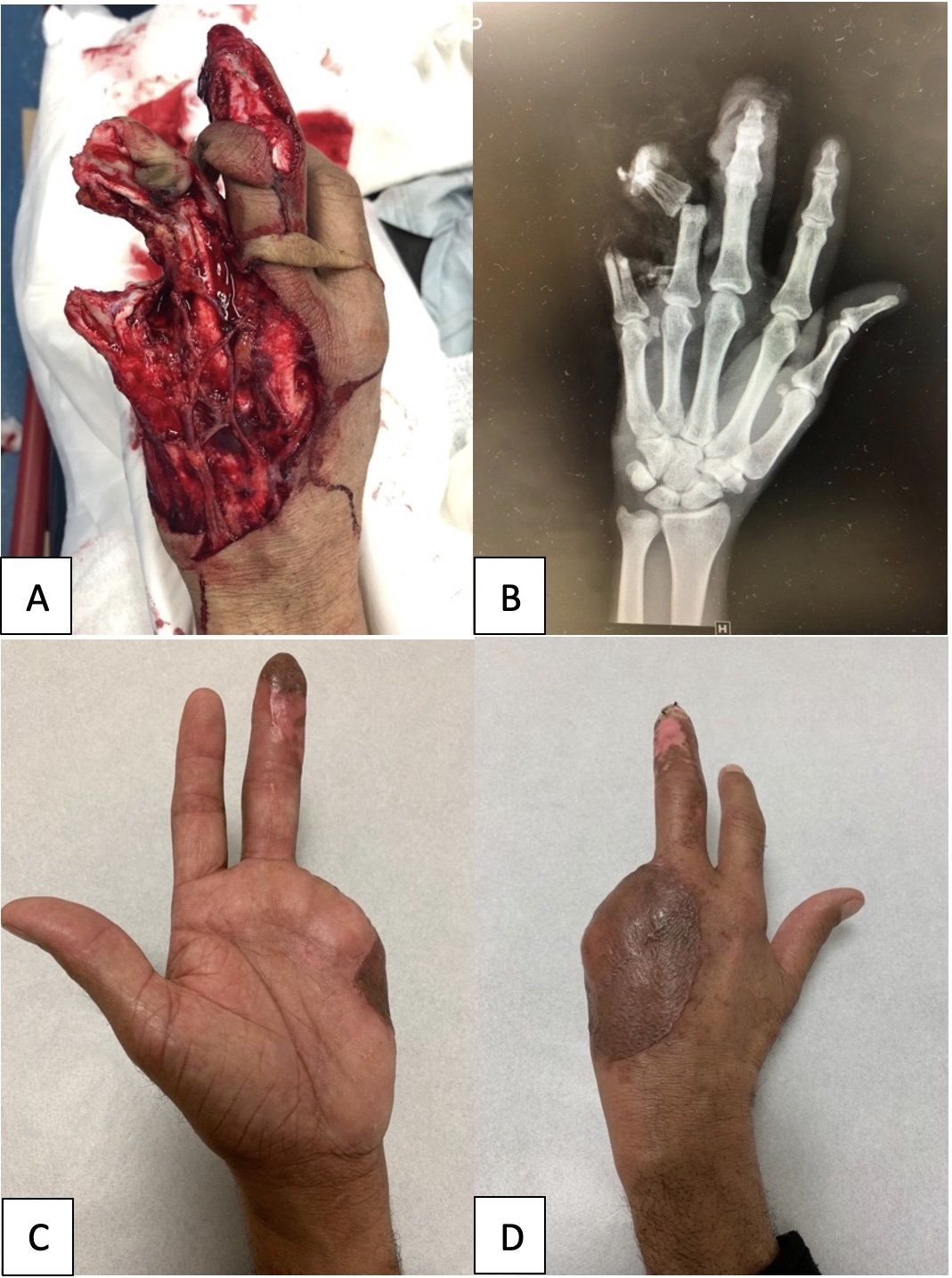
Relative indications have been a moving target in the literature. There seems to be some consensus for replanting single digits distal to Verdan’s zone II.4,5,7,9 At this level, the flexor digitorum superficialis has already been inserted on the middle phalangeal base. Thus, with only the flexor digitorum profundus in the sheath at that level, the replantation is done outside the dreaded “no man’s land.” A patient’s wishes based on their cultural mores or religious beliefs is another relative indication to proceed [FIGURE 1].8

Contraindications
As with the indications, there are absolute and relative contraindications. Replantation can be a long and complicated surgery with metabolic and physiological consequences. Thus, one of the strongest contraindications is the patient’s medical status.8,9 If the patient is in extremis and the surgery is likely to threaten their survival, it is strongly advised not to proceed. This can be seen with significant underlying medical issues or in unstable polytrauma patients.
Other absolute contraindications have to do with the condition of the donor or recipient site. If there is a segmental injury, unsuitable vessels for repair, severe mangling, avulsed vessels, or the ischemia time is outside of the window of viability, the replantation is not indicated [FIGURE 2].5,7–9

Relative contraindications are unclear and can be shifted either way based on the shared decision-making between the surgeon and the patient. Some of these include single-digit amputations in Verdan’s zone II and various patient factors.4,5,7,8 The latter can encompass psychiatric illness, self-inflicted digital amputations, smoking status, diabetes mellitus, peripheral vascular disease, and socioeconomic factors such as a patient’s ability to get postoperative rehabilitation or their ability to take time from work to recover properly.5,7,8 Each of these factors must be considered when deciding if an attempt at replantation is the right decision.
Predictors of Success
When planning for digital replantation, one needs to evaluate the chances of success and what factors play into that chance. In a retrospective review, Zhang et al. looked at 18 years of digital replantation in Canada. They showed that the overall success rate, defined as survival of the digit at discharge, was 71%. In their series, they noted that a sharp mechanism of injury, intact venous drainage (in partial amputations), a more proximal injury, and postoperative aspirin use were predictive of success. In their series, aspirin was the most commonly used postoperative anti-coagulant. The use of leeches or the need for re-exploration were predictive of failure.17 Similarly, Smith et al. reviewed seven years of digital replants in the United Kingdom and noted a 68% chance of success. In their series, a guillotine-type mechanism and shortening of the digit at the time of surgery increased the rate of success.18 Despite these consistencies, other studies have shown no significant predictive factors with respect to successful replantation.19 This speaks to the heterogeneity of these patients and why many factors need to be considered when indicating these patients for treatment.
Outcomes
Adding digital replantation to our armamentarium was a huge step over the time when zone II flexor injuries were a source of surgical trepidation. Despite that change and the predictors of technical success elucidated by Zhang et al. and Smith et al., success can only be determined if the outcome is well-defined.17,18 In the age of patient-reported outcomes, the definition of success is more complicated. Much research has been dedicated to this since the time of Komatsu and Tamai.
Recently, several well-done studies have looked at the outcomes of digital replantation and how they stack up against revision amputation. One of the more optimistic studies was published in 2019, when Chung et al. published a multicenter retrospective review of 338 patients, showing that the replantation group had a better MHQ, DASH, and PROMIS score. Based on their findings, they recommended that patients who have three digits amputated, a single finger distal to the proximal interphalangeal joint, or a thumb amputation undergo replantation surgery.20
Though that review supports replantation, there is some variability in the literature. In 2022, Bott et al. retrospectively reviewed five years of replantation at their center. In their series, the replanted digit achieved 58% of the range of motion of the contralateral digit. Grip and pinch strength were not significantly different; however, the pain was decreased in the replantation cohort, which is an important outcome measure.21 In 2021, a meta-analysis by Stone et al. compared the outcomes of 717 replanted digits with 1046 amputated digits. Though they showed an overall replantation survival rate of 85.3%, they were more tempered in their conclusions. They felt there is low-quality evidence that a thumb replant functions better, though it may be more clinically important. They also felt that there is low-quality evidence suggesting that single-digit replantation may improve outcomes, but they think this is less clinically significant.22
To muddy the waters even further, in another retrospective review by Billington et al. in 2021, it was shown that in their 76-patient cohort of 101 digits, the success rates are not always what we see in the literature. The success rate reported in their series was 33% of patients and 29% of digits, with a laceration being the most predictive factor for success.23
In reality, the success rate and outcomes probably lie somewhere in the middle of this milieu. What makes the data hard to digest in replantation is the variability of surgeons’ indications, patients’ cultural desires, and even the status of the medical center being a teaching or non-teaching hospital.4,5,7–9,24,25 Regional and teaching hospitals have a lower chance of success but have more attempts.24,25
The final point to consider in the adult population is what happens if the digit is not replantable, the patient is not a good candidate for surgery, or the patient chooses not to undergo the replantation. Revision amputations have been shown to have good outcomes as well. In Yuan et al.'s systematic review of 43 studies, revision amputations provided better outcomes than local flaps after traumatic amputations. Satisfactory, good, or excellent outcomes were reported in 91% of patients.26
When assessing the outcomes in children, one needs to consider that they have better healing potential and the ability to remodel and compensate over time. That said, the success rates are not as great as expected. This is due to several factors. One important aspect to consider is that the indications to attempt replantation are much more aggressive in children and may override certain contraindications in the adult population. Inherently, this will decrease the chances of success. In addition, the vessels are smaller, leading to technical challenges in the microvascular anastomoses. The narrow diameter of the vessel also predisposes the lumen to occlusion with vasospasm.7,8,16,27
Ethics
One non-clinical consideration for indicating a patient for replantation is the ethical implications of the situation. After such a traumatic injury, there are inherent challenges to obtaining truly informed consent. A patient’s ability to understand such a complicated procedure’s risks, benefits, and alternatives may be very poor. This is compounded by the fact that they do not have much time to consider their choices in such a stressful, time-sensitive environment. Attention must be given to appropriately counseling the patient in a calm environment to allow them to make a shared decision with the surgeon. This is particularly important in situations where indications and contraindications coexist, as we see in a thumb that has been crushed. Discussing the indication (thumb) and contraindication (crush) with the patient is critical to determine whether the indication will trump the contraindication or vice versa. Standardization of this process can also lead to better patient-centered care.28
CONCLUSIONS
Digital replantation has come a long way since the days of Komatsu and Tamai. The microsurgical technology and resources available to us now are far greater than those they had in the 1960s. This has undoubtedly led to our generation of surgeons being more capable and having more possible candidates for these procedures. That being said, the most considerable evolution in the last almost 60 years is the understanding we have developed from reflecting on our experiences and our patients’ experiences. Our indications have been sharpened, our outcomes are more predictable, and our expectations are better understood than they’ve ever been. We are also in the age of shared decision-making, which has honed our judgment. It will be interesting to see what the next half-century holds, especially with the advent of robotic-assisted surgery, improvements in prostheses, and the changing landscape of our healthcare system.
DECLARATION OF CONFLICT OF INTEREST
Dr. Vosbikian receives honoraria from The Journal of Bone and Joint Surgery Clinical Classroom for service as the section head of hand surgery, ePlasty for service on the editorial board, and Medartis for serving as course faculty.
DECLARATION OF FINANCIAL SUPPORT
The authors received no financial support for the preparation, research, authorship, and publication of this manuscript.
DECLARATION OF ETHICAL APPROVAL
Institutional Review Board approval was not required to produce this manuscript.
DECLARATION OF INFORMED CONSENT
There is no information (names, initials, hospital identification numbers, or photographs/images) in the submitted manuscript that can be used to identify any patients.