INTRODUCTION
The scaphoid is the most commonly fractured carpal bone, accounting for 11% of all hand fractures.1,2 They are often sustained from a fall on an outstretched hand with concomitant wrist hyperextension.3 Nonunion is a common complication associated with untreated scaphoid fractures.4 Patients who progress to nonunion can experience significant discomfort and may eventually require salvage procedures that decrease wrist function. Therefore, surgeons must correctly diagnose and treat scaphoid fractures to minimize complications.
There is still debate regarding the optimal treatment strategy for scaphoid fractures. Traditionally, the treatment of choice has been headless compression screw fixation.5 These screws are thought to both compress the fracture site while stabilizing the scaphoid through three-point fixation. The proximal and distal ends of the bone are captured by the threads, while the third point of fixation occurs within the waist of the bone.5 While the headless compression screw may stabilize many scaphoid fracture types, significant bone loss or comminution about the waist may compromise its fixation and thus increase the potential of a nonunion.1
Volar locked plating has recently been introduced and has been shown to have had success with nonunions.1,6,7 The plate addresses some of the shortcomings of the headless compression screw by providing more buttress support and rigidity in scaphoid fractures and with significant bone loss and scaphoid nonunions.1,5,7
INDICATIONS & CONTRAINDICATIONS
The indications for volar-locked plating of scaphoid fractures are an area of active research. Potential indications for locked volar plating of scaphoids include waist fractures with significant comminution or bone loss, unstable oblique waist fractures, and fractures in which the use of a headless compression screw may lead to excessive loss of scaphoid length.5,6 Additionally, volar locked plating is indicated in the setting of scaphoid nonunions with bone loss, humpback deformity, central cavitation after failed primary fixation with a headless screw, and established nonunions requiring extensive debridement.5,8
Contraindications to volar plate fixation of the scaphoid are not well-defined. However, a contraindication to volar locked plating may include substantial articular degeneration and/or patients with significant degenerative changes, such as scaphoid nonunion with advanced collapse.8
SURGICAL TECHNIQUE
RELEVANT ANATOMY
The scaphoid bone retains a complex three-dimensional structure described as resembling a boat, skiff, or twisted peanut, and its shape presents unique challenges to fracture fixation. The bone is often divided into three regions: the proximal pole (articulating with the scaphoid fossa of the distal radius and lunate), the waist, and the distal pole (articulating with the trapezoid and trapezium). The scaphoid is oriented in the carpus with an intra-scaphoid angle averaging 40 +/- 3 degrees in the coronal plane and 32 +/- 5 degrees in the sagittal plane.2,3 It is the only carpal bone that bridges the proximal and distal carpal rows and thus acts as a tie-rod to coordinate smooth carpal motion. Approximately 80% of the bone is covered by cartilage, limiting ligamentous attachments and vascular supply.2,3 The primary stabilizer of the carpus is the scapholunate interosseous ligament (SLIL), which is critical in maintaining normal carpal kinematics. The radioscaphocapitate (RSC) ligament originates from the volar radius, crosses the volar concavity of the scaphoid waist, and attaches ulnarly at the capitate. The RSC acts as a fulcrum around which the scaphoid rotates. The scaphocapitate and scaphotrapezial ligaments are the primary restraints of the distal pole. The predominant blood supply to the scaphoid occurs through retrograde flow via the dorsal carpal branch of the radial artery. Thus, proximal fractures are at an increased risk of dysvascularity and nonunion. Untreated displaced fractures of the scaphoid waist will usually flex as the volar bone is reabsorbed, yielding a “humpback” deformity, which, through simultaneous extension of the lunate, results in dorsal intercalated segment instability (DISI).
SURGICAL APPROACH
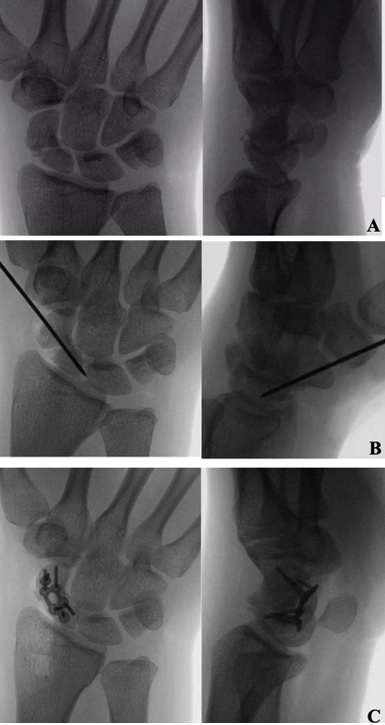
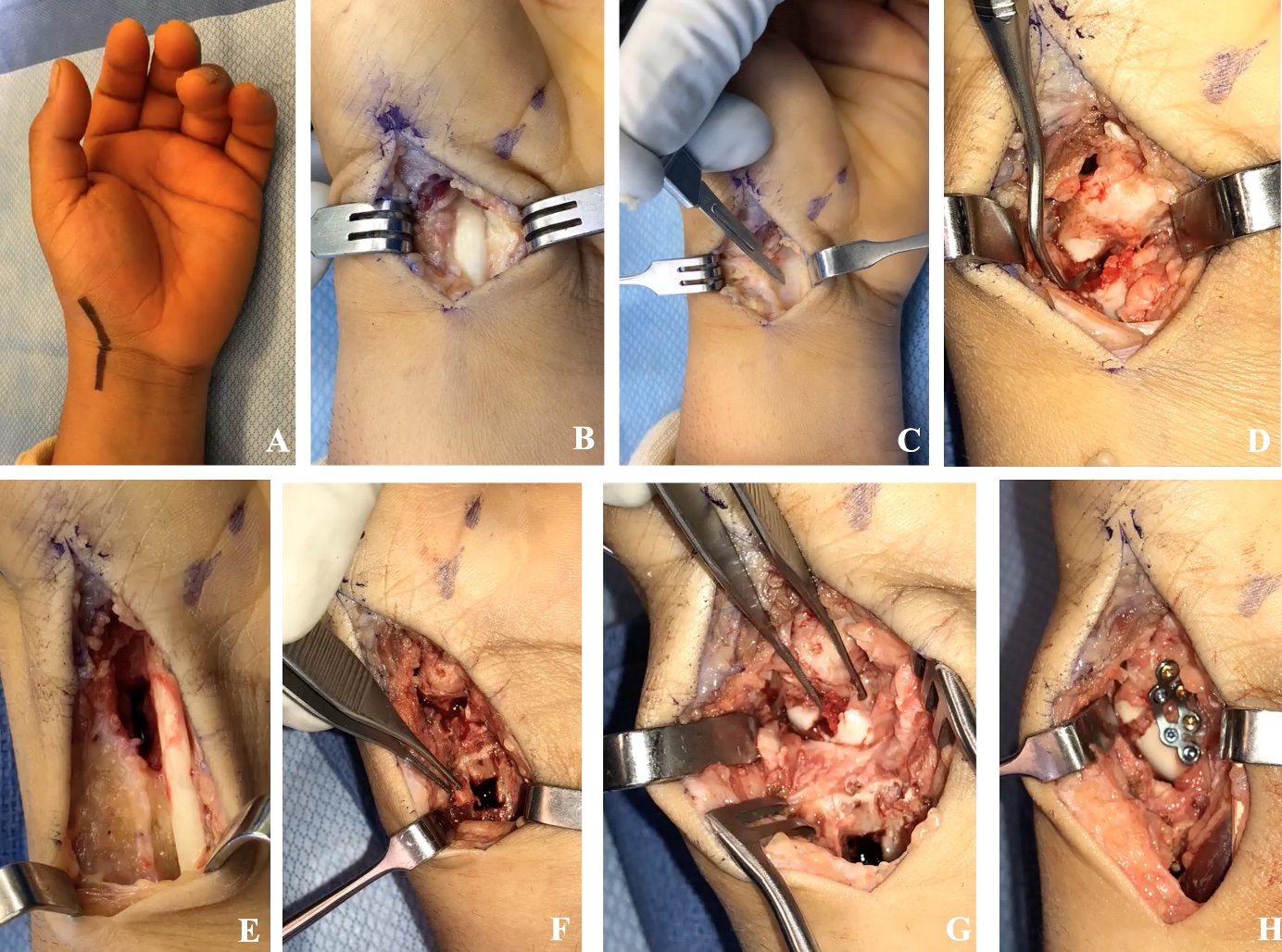
Fixation of scaphoids with a volar locking plate begins with the volar trans-flexor carpi radialis (FCR) approach to the scaphoid [Figure 1A]. The patient is positioned supine with a hand table, and tourniquet hemostasis is utilized. An incision is made in a hockey-stick configuration, centered over the FCR tendon at the wrist and angled across the wrist crease toward the base of the thumb [Figure 2A]. The FCR tendon sheath is incised and dissected distally, and the proximal thenar musculature is released for distal exposure [Figure 2B]. The FCR tendon is retracted radially, and the floor of the sheath is released, exposing the site of the capsular arthrotomy [Figure 2C]. The capsule and intracapsular ligaments are carefully divided and reflected sharply off the scaphoid. The RSC ligament is incised longitudinally to be repaired upon closure. The entire volar scaphoid is exposed.
_initial_fluoroscopic_images_depicting_a_comminuted_scaphoid_waist_fracture_with_a_flex.jpg)
FRACTURE REDUCTION & VOLAR PLATE FIXATION
Subsequent debridement of the fracture site is performed using a dental pick and curette [Figure 2D]. The scaphotrapezial and radiocarpal joints are identified to confirm the proper position. The fracture is then provisionally reduced by extending and supinating the distal fragment and pinning the fragments into place using a Kirschner wire [Figure 1B]. Once the deformity is reduced, a bony defect will typically present, especially post-debridement. In this case of an acute scaphoid fracture, a non-vascularized autogenous cancellous bone graft is chosen to fill the bony void. Multiple donor sites are available, such as the iliac crest, ipsilateral radial styloid, Lister’s tubercle through separate incisions, or the ipsilateral volar distal radius. In this case, the latter is chosen, and the graft is harvested by extending the surgical incision 2-3 cm proximally, exposing the volar distal radius proximal to the pronator quadratus [Figure 2E]. A corticotomy is performed [Figure 2F], and cancellous autologous bone is harvested and impacted into the scaphoid defect [Figure 2G]. Compression is not an option given the cancellous graft, so a pre-contoured 1.5 mm locking scaphoid plate (Medartis, AG, Basel, Switzerland) is selected for fixation. The plate is implanted by first using nonlocking, self-tapping cortical screws in the most proximal and distal holes. After compressing the plate to the bone, the remaining screws are placed in a locking fashion into both poles of the scaphoid. The two initial cortical screws are then replaced with locking screws so that both proximal and distal fracture fragments are subsequently filled with all locking screws [Figure 2H]. Fluoroscopy is used to confirm plate and screw placement, paying close attention to ensure screws are not violating adjacent joint articulations proximally and distally [Figure 1C]. Layered closure is performed by repairing the joint capsule, the RSC ligament, and finally, the skin. A complete list of pearls and pitfalls of volar plating are presented in [Table 1].
_hockey-stick_incision_centered_over_fcr_tendon_and_extending_radially_to_base_of_thumb.jpg)
POST-OPERATIVE MANAGEMENT
Post-operatively, patients are immobilized in a thumb spica splint for two weeks. They are then transitioned to a removable thumb spica brace or a thumb spica cast for eight to twelve weeks. During this time, they will remain non-weight-bearing. After that, patients will have a computed tomography (CT) scan of the fracture site to assess for union prior to discontinuing immobilization. This is particularly important for cases of scaphoid nonunion. If the CT confirms union, patients are advanced to a range of motion and lightweight bearing. If the fracture is not yet fully united on CT, the patient should remain immobilized, and an additional CT should be obtained to assess the progression of the union.
DISCUSSION
Volar locking plates can effectively stabilize acute scaphoid fractures and scaphoid nonunions. They provide consistent union rates and good functional outcomes. In a retrospective review of 34 patients with symptomatic scaphoid nonunions with segmental defects treated with a volar locking plate and cancellous bone graft, Putnam et al. demonstrated that all patients achieved union by 18 weeks with improvement in mean Disabilities of the Arm Shoulder and Hand (DASH) score, visual analog scale, and range of motion. The union rate may be attributed to the vascularized graft. However, the volar locking plate provides a rigid fixation and allows the graft to remain in the defect.9 Comparable rates of union are also found in Lemke et al.1 and Esteban-Feliu et al.10
Volar locking plates are not without complications. Lemke et al. demonstrated that 16 (57%) of 28 patients required hardware removal due to plate irritation.1 In a retrospective case series of 15 patients with symptomatic scaphoid nonunion treated with volar locking plate and bone graft, four patients developed complications: one with breakage of the plate and three with screw-backout.10 However, these complications should be cautiously considered given the small case number and lack of a control group.
The optimal treatment strategy for scaphoid fractures remains controversial. Volar locking plates stabilize areas of comminution and bone defects that do not allow for sufficient cortical contact and compression with headless compression screws. They are an option for scaphoid nonunions as they buttress the carpus and the bone graft. Volar locking plates are a promising modality for the treatment of scaphoid fractures and nonunions not amendable to headless compression screws.
Declaration of conflict of interest
Dr. Asif Ilyas receives royalties from Globus Medical, has been a paid faculty for Medartis, has received research funding from Axogen, and is a consultant for Globus Medical, Axogen, and Stryker. The other authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
This manuscript does not require ethical approval to report its findings.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.