INTRODUCTION
Primary management of open fractures involves adherence to Advanced Trauma Life Support (ATLS) guidelines, administration of systemic antibiotics according to the Eastern Association for the Surgery of Trauma (EAST) guidelines, and tetanus toxoid as needed within three hours of injury.1,2 Current guidelines from the American Academy of Orthopaedic Surgeons (AAOS) provide recommendations for preventing surgical site infection after extremity trauma.3 The Gustilo-Anderson classification of open fractures is well known and remains the most used classification system for open fractures.4 Gustilo, Mendoza, and Williams further divided type III open fractures into subdivisions in the order of injury prognosis worsening.5
Other classifications include the Orthopaedic Trauma Association Open Fracture Classification (OTA-OFC)6 and the Ganga Hospital Open Injury Scale (GHOIS).7 Each has benefits and drawbacks, but the Gustilo-Anderson system appears most often in literature.
Fractures resulting from civilian ballistic injuries represent a unique subset of open fractures that are becoming more common across the United States. Ballistic injuries in the civilian population are typically classified as low-velocity or high-velocity, with low-velocity injuries predominating.8–10 However, classifying these injuries using the Gustilo-Anderson classification is controversial among orthopedic traumatologists. Without a proper classification for ballistic fractures, developing treatment strategies remains challenging and underrepresented in the literature.11
This article investigates developments in treating open long bone fractures of the limbs, not including hands or feet. It provides an update to the current treatment guidelines, focusing primarily on recent findings in the prophylactic administration of antibiotics, methods for the delivery of local antibiotics, time to debridement, wound lavage techniques, and how these developments may influence the management of complications associated with open fractures with additional considerations for open fractures caused by civilian ballistic injuries.
METHODS
The population considered in this review identified all patients with open long bone fractures who were over the age of 19 who underwent medical treatment. We mainly focus on comparisons and outcomes of prophylactic antibiotic administration duration, time to debridement, irrigation practices, methods of local antibiotic delivery, and ballistic fracture management. To identify articles, a computerized literature search of the MEDLINE database was conducted utilizing Medical Subject Headings (MeSH) terms and other non-MeSH terms. Searches had a date filter and a filter that restricted results to only include human subjects applied to provide more current and relevant information. A filter was also set to include articles on clinical trials, pragmatic clinical trials, and review articles. The following are the searches used to gather literature: Fractures, Open [MeSH] AND Fractures, Open/classification [MeSH] AND Fractures, Open/therapy [MeSH]; Fractures, Open [MeSH] AND Antibiotic Prophylaxis [MeSH] AND Antibiotic Prophylaxis/adverse effects [MeSH]; Fractures, Open [MeSH] AND Therapeutic Irrigation [MeSH]; Fractures, Open [MeSH] AND Surgical Wound Infection [MeSH]; Fractures, Open [MeSH] AND Debridement [MeSH]; (Arm Bones [MeSH] OR Leg Bones [MeSH]) AND Fractures, Open [MeSH]; Antibiotic Prophylaxis [MeSH] AND Drug Resistance, Bacterial [MeSH] AND Surgical Wound Infection [MeSH]; Fractures, Open [MeSH] AND Fractures, Open/complications [MeSH] AND Therapeutic Irrigation [MeSH] AND (Fractures, Open/surgery [MeSH] OR Fractures, Open/therapy [MeSH]; Fractures, Open [MeSH] AND Anti-Bacterial Agents/administration and dosage [MeSH]; Fractures, Open/surgery [MeSH] AND Polymethyl Methacrylate [MeSH]; Fractures, Open [MeSH] AND Polymethyl Methacrylate [MeSH] AND Anti-Bacterial Agents [MeSH]; Surgical Wound Infection [MeSH] AND Polymethyl Methacrylate [MeSH] AND Local Antibiotic; Fractures, Open [MeSH] AND Antibiotic Bead Pouch; Fractures, Open [MeSH] AND Fracture Fixation, Intramedullary [MeSH]; Fractures, Open [MeSH] AND Fracture Fixation, Intramedullary [MeSH] AND Anti-Bacterial Agents [MeSH]; Fracture Fixation, Intramedullary [MeSH] AND Anti-Bacterial Agents [MeSH]; gunshot AND management AND fracture; gunshot AND antibiotic AND fracture. All gathered articles were subject to the same rigor for inclusion. A search query for open fractures associated with gunshot wounds was performed separately and similarly as described above.
The article title and keywords were reviewed following the literature search to determine relevance. Inclusion criteria included treatment of open fractures of long bones in an adult population. Exclusion criteria included publication in a language other than English, treatment of non-human subjects, the inclusion of gunshot wounds in the classification of open fractures, and treatment of patients younger than 19. The literature was further dissected with an abstract and article review, keeping in mind the inclusion/exclusion criteria. Included literature was classified according to the level of evidence (according to the guidelines in the Journal of Orthopaedic Trauma12) and then divided according to the relevant topics of this review: duration of prophylactic antibiotic administration, time to debridement, irrigation practices, methods of local antibiotic delivery, and other management strategies. Review articles were considered in the scope of our review. Utilizing the literature, a protocol for managing all open fractures was created.
RESULTS
Debridement
The near-consensus of articles challenges the previous paradigm of a “6-hour rule,” allowing for delays up to 24 hours after the injury to ensure the patient is optimized for surgery and appropriate personnel and equipment are present.13–21 Southam and Archdeacon argue that aggressiveness and completeness of debridement are important factors in open fracture management; however, a retrospective review by Ricci et al. found that patients undergoing more aggressive debridement did not have better outcomes compared to those with a less aggressive debridement.22,23 Johal et al. performed a propensity score-based analysis of the Fluid Lavage in Open Fracture Wounds (FLOW) trial data set, finding that patients undergoing earlier irrigation and debridement were associated with a higher proportion of re-operation, which disappeared when the propensity match was applied to account for severe injuries.24 There is currently a moderate recommendation from the AAOS, suggesting that patients with open fractures be brought to the OR for debridement and irrigation as soon as possible, ideally within 24 hours post-injury.3
Irrigation
New evidence for optimizing irrigation strategies relies heavily on data from the Fluid Lavage in Open Fracture Wounds (FLOW) trial. The FLOW trial found that very low pressure irrigation with normal saline had better outcomes.25 Kortram et al. published a systematic review of risk factors for deep infections, and the only operation-related factor was the use of pulsatile lavage.26 While there is no “ideal” irrigation solution, copious normal saline has been determined to be the best option to irrigate open fractures due to its availability, sterilizability, and facilitation of wound healing compared to other non-isotonic or cytotoxic agents.27,28 Sprague et al. expanded the FLOW trial with limited new findings.29 There is a strong recommendation from the AAOS for using saline (without additives) to manage open wounds in extremity trauma.3
Local Antibiotics and Wound Care
Local antibiotics can be administered through vancomycin powder, polymethyl methacrylate (PMMA) beads impregnated with aminoglycosides, and intramedullary nails (IMN) coated with antibiotic-impregnated cement, among other options.30–39 The Major Extremity Trauma Research Consortium (METRC) published the final results of the VANCO trial in the Journal of American Medical Association (JAMA) in 2021.36 They found that administering intra-wound vancomycin powder at the time of definitive fracture fixation significantly reduced (3.4%) the risk of gram-positive deep surgical site infection (SSI). Regarding PMMA beads, Craig et al. found them to be a common and safe practice in managing open fractures as long as the beads could be removed later.30 Seligson and Berling recommend stringing beads together to facilitate removal.31 Metsemakers et al. conducted a small retrospective review to determine the effectiveness of a less common polymer used in cementing for IMN coating, Poly-D, L-Lactic Acid (PDLLA), which had a 100% effectiveness in preventing infection in this small sample.34 Morgenstern et al.'s investigation determined that local antibiotics lowered infection rates when added to the regimen of systemic prophylaxis.38 Furthermore, studies on nanoparticles and recombinant human BMP-2 suggest that these treatments may result in higher healing rates, which requires further investigation.39,40 There is currently a moderate recommendation from the AAOS regarding local antibiotic administration, suggesting that local antibiotic prophylactic strategies, such as vancomycin powder, tobramycin-impregnated beads, and gentamicin-coated nails, may be beneficial.3
With regard to wound therapy, recent comparative studies on negative pressure wound therapy (NPWT) versus conventional wound care situationally support the use of NPWT.41–43 The AAOS currently has a strong recommendation for closing an open wound when feasible without any gross contamination and additionally has a strong recommendation stating that NPWT does not confer any advantage when compared to sealed dressings for open fracture management as it does not decrease wound complications or amputations.3 There is a moderate recommendation from the AAOS regarding silver-coated dressings, which are not suggested to improve outcomes or decrease pin site infections.3
Systemic Antibiotics
Over the last decade, management of open fractures with prophylactic antibiotics has been a mainstay of treatment. However, despite level I and II evidence set forth by the EAST Guidelines, questions remain regarding the optimal antibiotic type, dosage, and duration of treatment. The EAST Guidelines recommended with level I evidence are as follows:
-
Systemic antibiotics with gram-positive coverage should be initiated immediately after injury.
-
Additional gram-negative coverage should be added for type III fractures.
-
High-dose penicillin should be added for injuries with fecal or potential clostridial contamination.
-
Fluoroquinolones offer no advantage compared to cephalosporins/ aminoglycosides.
Level II evidence
-
In type III fractures, antibiotics should be continued for 72 hours or no more than 24 hours after wound closure.
-
Once daily aminoglycoside dosing is safe and effective for type II/III fractures.44
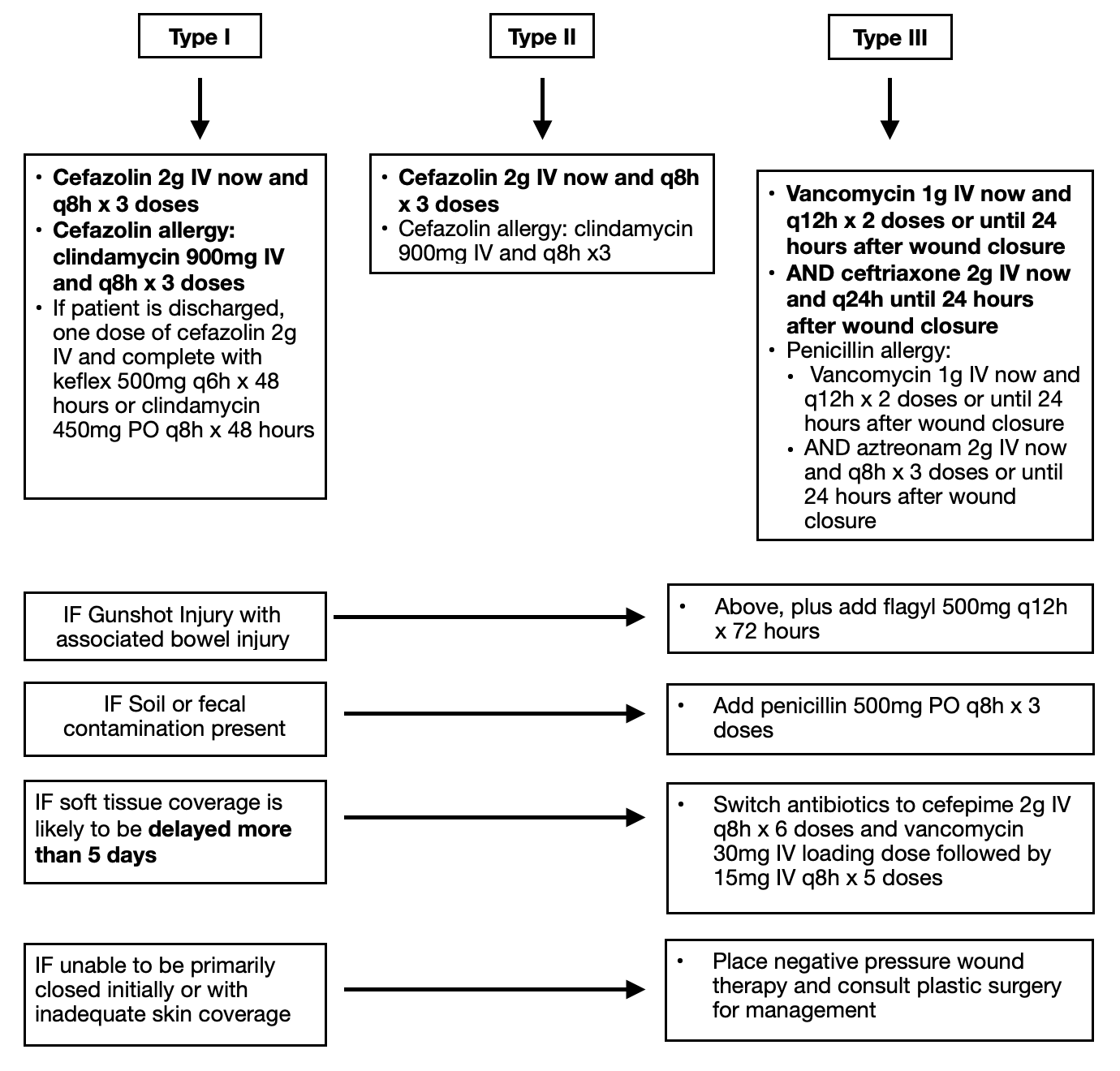
The recommendation for antibiotic administration with gram-positive coverage as soon as possible continues to accrue support from the literature. Furthermore, timely and appropriate antibiotic administration appears to be the most important variable affecting a patient’s risk of infection secondary to the severity of the injury itself.21,40,45–51 Intravenous (IV) cefazolin is the clear gold standard of antibiotic prophylaxis in open fractures, and substantial evidence supports administration as early as possible, ideally within one hour of injury. The usage of antibiotics with gram-negative coverage and broad-spectrum antibiotics has received increased attention recently. Multiple studies advise against the use of aminoglycosides, such as gentamicin, because of potential acute kidney injury (AKI), favoring aztreonam, ceftriaxone, or cefepime.19,41,52–56 Moreover, multiple studies have found that adding or removing gentamicin does not influence infection risk.19,53 However, gentamicin is still a safe and effective option in select patients with low risk of AKI who are adequately resuscitated.49 Sagi and Patzakis argue that routine use of broad-spectrum antibiotics is not always indicated, even in type III injuries, as most gram-negative infections are often hospital-acquired secondary to delayed wound closure.49,50 In light of this information, they recommend all open fractures receive gram-positive coverage. In contrast, gram-negative coverage with third to fifth-generation cephalosporins is appropriate for type III injuries that are unlikely to achieve soft tissue coverage within five days.49,50 Messner et al. performed a comprehensive literature review and meta-analysis with data from the 1970s to 2017 to evaluate the optimal duration of antibiotic prophylaxis for open fractures, finding antibiotic treatment beyond 72 hours did not further reduce infection.57 The AAOS currently provides a strong recommendation for patients with major extremity trauma undergoing surgery to receive cefazolin or clindamycin, except in the case of type III open fractures, where additional gram-negative coverage is recommended. Furthermore, the AAOS has a moderate recommendation for the early delivery of antibiotics to lower the risk of deep infection, and the use of preoperative antibiotics is suggested to prevent infection in the operative treatment of open fractures [Figure 1].3

Ballistic Injury
Open fractures resulting from gunshot injuries are open fractures because, by definition, communication between the fracture and the outside environment is created. However, these injuries may present with significant heterogeneity and are commonly reported to have significantly lower infection risk compared to traditional open fractures.8–10 Su et al. report that open fractures to the tibia caused by low-velocity gunshot wound (LVGSW) carried an infection rate of 2.3%, contrasting the 25%, 19.5%, and 47% infection rates that follow Gustilo-Anderson type II, IIIA, and IIIB, respectively.58 They also report significantly higher nonunion rates in non-gunshot related open tibia fractures. Metcalf et al. expanded the work of Su et al. by increasing sample size and standardizing fracture fixation methods, finding infection rates of 1% for closed trauma fractures (CTF), 9% for gunshot wound (GSW) fractures, and 20% for open trauma fractures (OTF).59 Moreover, nonunion rates were 8% for CTF, 15% for GSW, and 20% for OTF. When stratifying GSW fractures into two groups based on soft tissue injury, an increased nonunion rate (15% versus 50%) was found with more severe injury. Lee et al. studied nine years of gunshot-induced tibia fractures at multiple study centers, seeking to elucidate complications.60 Nearly half of these injuries developed a complication, including 14% infections, 27% wound complications, 20% nonunion, 9% hardware breakage, and 26% revision surgery. Deep debridement was the only factor they found to be associated with deep infection. Graham et al. cautioned drawing valid conclusions regarding ideal surgical management despite reported low infection risk for both low and high-velocity GSW, as no study used a validated scoring system.61 A survey of members of the Orthopedic Trauma Association (OTA) showed that most orthopedic traumatologists did not believe the Gustilo-Anderson classification applied to ballistic fractures and did not use it to guide treatment.62 Woolum et al. investigated whether antibiotic choices influenced clinical outcomes, grouping subjects into three treatment cohorts: narrow spectrum gram-positive coverage, expanded gram-negative coverage, or a fluoroquinolone. There was no difference in infection at two weeks post-operatively between groups. Still, the expanded gram-negative group had a longer stay and was more likely to be colonized by multi-drug-resistant bacteria.63 However, retrospective design and failure to account for cohort baseline differences are notable limitations of this study. Formal irrigation and debridement practices in civilian GSW fractures may differ from open fractures secondary to trauma. Two studies with low levels of evidence suggest that irrigation and debridement may not reduce infection rates. Donnally et al. caution against irrigation and debridement in patients at high risk for infection, such as smokers or AO/OTA 42-A fractures.64 Sathiyakumar et al. performed a literature review to elucidate management strategies for open ballistic fractures using only what they deemed to be high-quality data.65 Based on the evidence, they suggest that superficial debridement is a safe alternative to extensive debridement for non-operative LVGSW fractures with no gross contamination, large soft tissue defect, vascular injury, or compartment syndrome, but were not able to form recommendations for more severe injuries and tentatively recommend extensive irrigation and debridement for HVGSW. Moreover, they recommend a short course of prophylactic oral cephalosporin for LVGSW and 48-72 hours of broad-spectrum coverage for GSW fractures with communicating bowel injury. These recommendations are echoed by Laubscher et al. and Maqungo et al.8,10 Bartlett et al. suggest that 48 hours of Intravenous (IV) cefazolin, one dose of intramuscular (IM) cefonicid, 72 hours of IV cefepime and gentamycin, or oral ciprofloxacin are all safe and effective. Evidence from Ordog et al. had similar success with local wound care and topical antibiotics alone.66 There are currently no AAOS guidelines for the management of ballistic fractures.
CONCLUSION
Recent literature has unanimously emphasized the immediate administration of antibiotics to reduce the risk of infection from open fractures, with many even recommending administration by first responders in the field. Early antibiotic administration is the most important factor in reducing infection risk for open fractures. Cefazolin is the current gold standard for treatment. While rarer, adding penicillin for fecal or farm contamination is still recommended. Adding gram-negative coverage is recommended for more severe open fractures, especially if the injury precludes primary closure after initial irrigation and debridement. The optimal antibiotic, timing of administration, and treatment duration remain areas for further investigation. Prophylactic treatment with ceftriaxone, cefazolin plus aztreonam, vancomycin plus cefepime, or clindamycin plus aztreonam for 24 to 72 hours have all been proposed as reasonable prophylactic strategies. Still, the evidence on the comparative efficacy of these treatment regimens is lacking, and they are by no means the only options. Prolonged antibiotic prophylaxis (beyond 24 hours after wound closure) does not confer any additional benefit to short courses.
The timing of irrigation and debridement is still a factor, and, in general, more severe injuries benefit from earlier irrigation and debridement. However, irrigation and debridement with copious, sterilized, isotonic saline at low pressures may be safely delayed up to 24 hours to ensure appropriate personnel and resources are available.
Based on limited available evidence, we recommend treating ballistic open fractures following open fracture protocols with regard to antibiotics. Often, these injuries do not require extensive irrigation and debridement unless severe soft tissue injury or contamination is present or the bullet trajectory passes through a joint or the abdominal viscera. Most often, low-velocity missiles cause civilian gunshot wounds, and non-operative fractures can be safely managed in the outpatient setting after receiving a short course of antibiotics and tetanus booster if indicated. An iatrogenic injury should be limited, and therefore, retained bullet fragments should only be immediately removed if they are easily accessible, intra-articular, or causing neurovascular or related compromise.
Fractures from a ballistic mechanism are becoming more prevalent throughout the US. Utilizing the literature above, we set forth a suggested management pathway for open fractures, including ballistic injuries.
Declaration of conflict of interest
The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of funding
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of ethical approval for study
This manuscript does not require ethical approval to report its findings.
Declaration of informed consent
There is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.