
INTRODUCTION
Necrotizing fasciitis is a rare yet limb- and life-threatening infection of the subcutaneous tissues. While the microorganisms (Group A Streptococcus, Staphylococcus aureus, Klebsiella pneumoniae) frequently associated with this entity are familiar, necrotizing fasciitis is unique in its location, residing in contained and expansive fascial planes.1,2 Patients may present with severe pain, swelling, skin discoloration, bullae, subcutaneous emphysema (if secondary to a gas-producing organism), and hemodynamic instability if there is a resultant systemic inflammatory response syndrome.1 Commonly attributed risk factors for developing necrotizing fasciitis include an immunocompromised state (diabetes, immunodeficiency conditions, cancer) and external exposures that introduce bacterial pathogens (intravenous drug use, insect bites, trauma).1 Although not classically associated, lymphedema in an extremity may create an immune-deficient environment, which can be a risk factor for necrotizing fasciitis.3 This report presents findings from a unique case of culture-negative but pathology-confirmed necrotizing fasciitis of the forearm in a patient with lymphedema secondary to lymph node dissection for treatment of primary breast adenocarcinoma.
CASE REPORT
Patient Information
The patient is a 62-year-old female with a past medical history of left breast adenocarcinoma status post left breast mastectomy, radiation, and chemotherapy treatments with resultant chronic left upper extremity lymphedema who presented to the emergency department with ten hours of fevers, chills, and left hand and forearm erythema and “tightness.”
Clinical findings
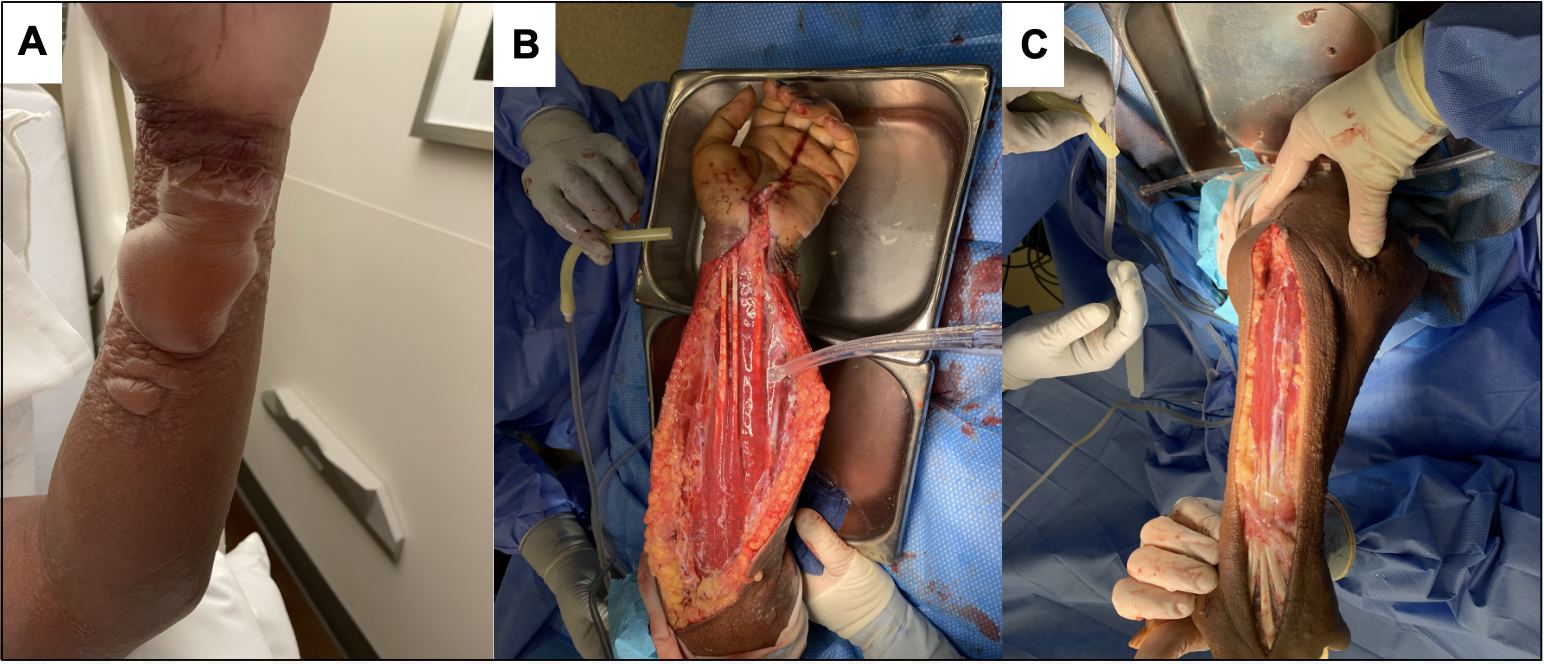
The patient had a temperature of 101.5 degrees Fahrenheit, a heart rate of 116 beats per minute, and a blood pressure (mmHg) of 125/81 (systolic/diastolic). She was examined by the emergency medicine department and was found to have left hand erythema and decreased range of motion, with fluid-filled blisters, noted on the volar aspect of her left wrist. She was admitted to the medicine service with a working diagnosis of left upper extremity cellulitis and was started on scheduled intravenous vancomycin and continuous intravenous fluids. Around noon the day after admission, the orthopaedic hand surgery service was consulted to evaluate the left wrist for a presumed diagnosis of septic arthritis. Upon examination, the patient’s blood pressure was 96/54, and the edematous left upper extremity also had extensive erythema with multiple bullae on her left hand and forearm [Figure 1]. She endorsed global tenderness to palpation in the left forearm and hand with increased pain upon passive extension of the fingers. There was also mild but generalized decreased sensation with paresthesias throughout the ipsilateral hand. Her blood cultures also turned positive for Streptococcus dysgalaciae overnight using a rapid polymerase chain reaction (PCR) assay. The patient’s serum laboratory findings at the time of orthopaedic consultation included a white blood cell count (WBC) of 20.3 (103/µL), C-reactive protein (CRP) of 246 (mg/L), hemoglobin of 13.5 (g/dL), and sodium of 135 (mEQ/L), amounting to a Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score of 6 which signified a high risk of necrotizing fasciitis.4
Therapeutic Intervention
Because of these stark clinical and laboratory findings, the patient was indicated for emergent surgery within two hours of orthopaedic consultation. Specifically, she underwent extensile fasciotomy with fasciectomy, radical soft tissue debridement of devitalized soft tissue, carpal tunnel release, and thorough washout of the left upper extremity [Figure 1]. Upon initial exploration of the fascial layer, copious ‘dishwater fluid’ extravasated from the forearm. The fascia was gray and friable from the wrist throughout the volar and dorsal forearm. The debridement was carried from the volar and dorsal hand through the volar and dorsal forearm and into the upper arm. The necrotic fascia was excised until only the proximal, healthy-appearing fascia remained. A slow lavage using cystoscopy tubing was used to irrigate the wound with multiple liters of normal saline. The wounds were left open and packed with wet-to-dry dressings and wrapped with kerlix and elastic bandages. The following day, the patient underwent a second-look irrigation and debridement of the left upper extremity, which showed little to no residual infection and overall healthy appearing soft tissue. A few low-tension wounds were closed primarily with nonabsorbable sutures, and the remaining sites were again left open and covered with wet-to-dry dressings.

Diagnostic Assessment
Tissue samples from the fascia were sent to pathology. Histological examination of the tissues confirmed the diagnosis of necrotizing fasciitis, demonstrating acute inflammation and necrosis of the fascial tissues [Figure 2].
_image_of_deep_tissues._b__high_power_(100x)_image_of_deep_tissues.png)
Outcomes
After four days of wet-to-dry dressing changes, the patient’s dressings were replaced with a deep wound vacuum-assisted closure device (negative pressure wound therapy) to promote granulation tissue development. After two weeks with vacuum-assisted closure, the patient underwent split-thickness skin grafting. After 27 days in the hospital, the patient was discharged home.
DISCUSSION
This case report presents findings from a unique culture-negative but biopsy-proven necrotizing fasciitis affecting the upper extremity that was successfully treated with early operative debridement. The strengths of this case report include (1) demonstrating how microorganism gram stain and culture can be negative despite suggestive findings in the operating room and (2) identifying the role of lymphedema as a risk factor for developing necrotizing fasciitis in the absence of trauma or wounds. The primary limitation of this report is that while specific findings were attributed to necrotizing fasciitis, they could not be externally validated for all scenarios. Thus, clinicians must maintain a broad differential for each patient to minimize under or over-treatment. The second limitation was that no objective or imaging findings confirmed the patient’s primary risk factor of chronic lymphedema.
While necrotizing fasciitis is a universally recognized ‘cannot-miss’ diagnosis, up to 75% of the cases reported in the literature are misdiagnosed because the window can be as short as 24 hours within the patient’s presentation.5 The patient in this case report lacked some of the typical risk factors reported in the literature, including recent trauma or wounds (30-70% of the time), recent surgery near the affected site (3-4%), diabetes (~45%), consumption of raw or uncooked seafood, or exposure to marine bacteria including Vibrio spp., Aeromonas spp., or Shewanella spp.5,6 However, the patient did have a history of chronic lymphedema on the ipsilateral side secondary to a history of breast adenocarcinoma treated with radical mastectomy, chemotherapy, and radiation. While the rate of association between chronic lymphedema and necrotizing fasciitis is unknown, Hara et al. previously presented a case of a 70-year-old woman with a history of total hysterectomy and pelvic lymphadenopathy for uterine cancer with subsequent chronic lower extremity lymphedema confirmed with lymphoscintigraphy that went on to develop rapidly progressing necrotizing fasciitis of the left thigh and lower leg.3 The patient initially presented with 1-day of extremity swelling and erythema, systemic symptoms including fever, diarrhea, and vomiting that quickly progressed to septic shock with renal and heart failure. The second day demonstrated significant bullae of the extremity, and later computed tomography imaging would confirm the presence of gas and fluid accumulation in the fascial planes, for which the patient was successfully treated with extensive debridement two days after presentation. Similar cases have even been presented in patients with a history of elective breast reconstruction in the absence of cancer.2
Interestingly, one of the unifying signs associated with necrotizing fasciitis is blister or bullae formation, much like the patient in the present report. Wang et al. retrospectively reviewed a relatively large cohort of 22 patients with necrotizing fasciitis. Based on clinical findings, they divided them into three presentation stages (early, intermediate, and late).7 They found that bullae and blister formation (a proxy for critical skin ischemia secondary to necrolysis of vascular perforators to the skin) around 37 hours after presentation were the hallmarks of intermediate to severe disease. Furthermore, systemic symptoms, including fevers (up to 40% of the time), hypotension (21%), and tachycardia (59%), while commonly associated with necrotizing fasciitis, are not essential for early diagnosis and often represent an impending rapid decline in the patient’s overall status.6 Cantarella et al. presented a case of necrotizing fasciitis of the gluteal musculature secondary to intramuscular injection of muscle relaxants where the patient went into septic shock peri-operatively despite reaching the operating room for debridement within 5-hours of presentation and prompt administration of broad-spectrum intravenous antibiotics.8 Cases like these underscore that timely diagnosis of necrotizing fasciitis means being ahead of the clinical findings rather than waiting for them to occur. In the present case report, the patient was presented to and fully treated at an acute suburban hospital 45 minutes away from a tertiary/quaternary care center in a major metropolitan area. While not all hospitals have immediate access to orthopaedic and plastic reconstructive care, initial operative debridement for necrotizing fasciitis should not be delayed for transfer to a higher level of care. Kay et al. presented a case series of 5 patients with necrotizing fasciitis diagnosed and successfully treated with operative debridement at a rural Australian hospital with limited subspecialty access.9 In this cohort, the average surgical referral occurred within 2.2 hours of triage and operative intervention within 7.2 hours. There were no mortalities in this cohort, and all five patients were ultimately stabilized and then transferred to a tertiary care center for definitive management for additional debridement or plastics reconstruction.9
The present case report demonstrates how carefully piecing together a constellation of risk factors and early signs and symptoms led to the timely identification of necrotizing fasciitis with limited laboratory and imaging findings. Additionally, this case shows that wound cultures can still be negative despite clear signs of infection during diagnosis and operative debridement. The absence of positive bacterial cultures at first debridement can lead to second-guessing, given the pressure clinicians face when balancing the consequences of differentiating necrotizing fasciitis from other non-severe soft tissue infections. As highlighted in this report, necrotizing fasciitis starts with non-specific symptoms of pain and swelling, which rapidly transform into systemic signs of vital instability without warning. Diagnosing necrotizing fasciitis in the early clinical course is ultimately elusive. However, this case report should give clinicians confidence that they can successfully manage this entity in a timely manner by maintaining a heightened index of suspicion and recognizing the unique and even atypical aspects of each case.
DECLARATION OF CONFLICT OF INTEREST
The authors do NOT have any potential conflicts of interest related to the content presented in this manuscript."
DECLARATION OF FUNDING
The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
DECLARATION OF ETHICAL APPROVAL
The affiliated institution does not require ethical approval for reporting individual cases.
DECLARATION OF INFORMED CONSENT
There is no information (names, initials, hospital identification numbers, or photographs / images) in the submitted manuscript that can be used to identify patients. Informed consent to review, write up, and public this case was obtained from the patient.
When asked for the patient’s perspective on the treatments she received for her illness, she noted: “My care was very good, and I have no complaints. I’m grateful that you saved my life.” Informed consent was secured prior to submitting and presenting this Case Report.